The Abdominal Plain Film- Differentiating Large and Small Bowel
Differentiating stomach, small bowel and large bowel anatomy on the abdominal plain film can be a deceptively difficult task. In the presence of pathology, large bowel can mimic small bowel and vice versa. This page covers some methods for differentiating GIT anatomy on plain film. It would be prudent to peruse the Abdominal Plain Film Terminology page before reading on.
Summary of Characteristics
Characteristic
Stomach
Small Bowel
Large Bowel
Position
- Left Upper Quadrant
- Fundus directly under left hemidiaphragm
- obliquely orientated
- attached to transverse colon via gastro-colic ligament (variable in length)
- Central abdomen
- circumferential- the large bowel tends to frame the small bowel
Contents
- fluid and air
- fluid-like succus entericus and air
- faeces of variable consistency from liquid to hard formed
Mucosal/Wall Pattern
- Rugal folds (can be effaced if distended)
- Can have a random faceted/tessellated appearance when air-filled (but not dilated).
- Encircling valvulae conniventes visible depending on degree of air filling/distention.
- Valvulae conniventes more widely spaced in ileum
- Wall pattern can be effaced if distended
- Haustral folds interspaced with Plicae semilunaris
- Wall pattern can be effaced if distended
Size
- Variable
- Up to 30mm
- Up to 50-60mm
- Up to 90mm for the caecum
The 3,6,9 Rule
The maximum diameter of the bowel is shown below
Maximum Normal Diameter small bowel 30mm large bowel 50-60mm caecum 90mm
The 3,6,9 rule is a very useful guide to determining when the bowel is dilated. It can also be useful in distinguishing between small and large bowel. For example, if the bowel measures 90mm in diameter it is highly unlikely to be small bowel.
The Stomach

The stomach does not commonly present difficulties in identification on a supine abdominal plain film despite its variable appearance and position. The stomach can be positioned high and horizontal or vertical and long, dropping down into the pelvis. The stomach will not contain formed faecal material. The stomach may be collapsed and largely empty or may be air-filled or fluid-filled, or both.
The characteristic oblique position of the stomach with a visible rugal fold as seen in this image(left) makes for easy identification(white arrow).
This image is taken from a barium meal series. The gastric rugae are clearly visible.


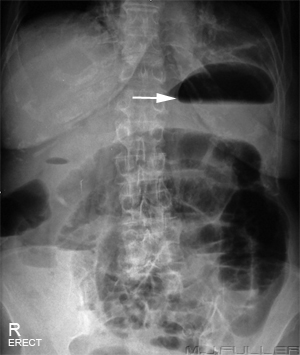
The stomach can be equally characteristic in its appearance on an erect abdominal plain film. The often smoothly radiused contour of the air-filled gastric fundus under the left hemidiaphragm and the characteristic air-fluid level make for easy identification.

The Small Bowel
Normal Gasless Small Bowel

This patient appears to have a gasless small bowel. Fluid-filled loops of small bowel are present but are never as well visualised as air-filled loops.
There is debate regarding what is a normal amount of small bowel gas. Gas enters the small bowel during eating and drinking. Some people habitually air-swallow while others air-swallow at times of stress or when they are in pain. If the patient is air-swallowing at a higher rate than the small bowel can absorb the air, it will be visualised in the bowel. Some texts will claim that up to seven fluid levels in the small bowel on an erect abdominal film can be normal. Most texts quote a more conservative figure.
I have heard it said that any air visualised in the small bowel is abnormal. I find this assertion hard to support.
Don't confuse gasless with featureless. A featureless abdomen can be a result of tumour or ascites. This patient has a gasless rather than featureless abdomen. Note that the renal, liver, psoas muscles and urinary bladder outlines are visualised
Note that this abdominal film is not guaranteed to be normal. It could represent an early gasless small bowel obstruction. Clinical correlation required.

Gasless Small Bowel Obstruction
You could be forgiven for thinking that this patient has been drinking dilute gastrografin. This appearance is a gasless small bowel obstruction and the opaque looking small bowel loops (white arrow) are filled with normal succus entericus rather than gastrografin. If you compare this image with the gasless small bowel image above you can see that this small bowel is significantly more prominent.
There can be difficulty in distinguishing an early gasless small bowel obstruction from a normal appearance of the small bowel in someone who has just eaten a large meal.
Clinical correlation and follow-up imaging will usually provide confidence in the diagnosis.

Normal Air-filled Small Bowel
This is an AP lumbar spine image on a patient who presented with back pain. It would be reasonable to assume that this patient is unlikely to have acute abdominal pathology (although not completely excluded). The appearance of the small bowel visualised in the left iliac fossa is a result of normal air swallowing (white arrow). The bowel diameter has been measured at 30mm which is the upper limit of normal. This patient is likely to be in pain and is therefore more likely to air-swallow resulting in this appearance.
The appearance has been likened to crazy paving or the pattern on a giraffe. It appears as an interlocking, random, tessellated pattern.
Crazy Paving.............................................................Giraffe!
Moderately Dilated Air-filled Small Bowel
The small bowel demonstrated in this image is moderately dilated (36mm). There is evidence of loss of the normal random tessellated pattern associated with undilated air-filled small bowel. Instead, the bowel is showing signs of a pattern which is more organised rather than random. There are, for example, multiple loops of small bowel which have become aligned or parallel.
This appearance is typical of an early small bowel obstruction or a partial small bowel obstruction.




Severely Dilated Air-filled Small Bowel (Coiled Spring Sign)
The coiled spring appearance only occurs in dilated air-filled small bowel. It also is most noticeable in the jejunum where the valvulae conniventes are tightly spaced.


String-of-Pearls Sign
The curvi-linear arrangement of air bubbles visualised on this image is known as the string of pearls sign. The appearance is considered to be diagnostic of obstruction (as opposed to ileus) and is caused by small bubbles of air trapped in the valvulae of the small bowel.
Source: Baker, S.R. The Abdominal Plain Film,p161
A similar appearance is sometimes seen in the large bowel but can usually be differentiated by the fact that the gas bubbles are larger and have flat under-surfaces


The Large Bowel
Haustral Pattern
The air-filled large bowel commonly features a haustral pattern as shown. The haustral folds are thicker than the valvulae conniventes of the small bowel. They also commonly do not appear to completely traverse the bowel. This distinction is unfortunately unreliable- air dilated large bowel can have a haustral pattern that does traverse the bowel. Furthermore, in some cases, the haustral pattern can be lost completely.
The large bowel will normally contain air. This is air produces partly from fermentation processes within the large bowel. The transverse colon and sigmoid colon are the least dependent segments of the large bowel in the supine position and will tend to fill with air.
Bowel Contents
You can't better faeces when it comes to positive identification of the large bowel. Neither the stomach nor the small bowel contains faeces. The arrowed bowel does not demonstrate a clearly identifiable wall pattern...doesn't matter... it contains faeces...must be large bowel.


The Large Bowel String of Pearls Sign
The large bowel has its own version of the small bowel string of pearls sign. Because the plicae semilunaris of the large bowel are larger than the valvulae of the small bowel, the pockets of air tend to be larger. Also, because they are larger in the large bowel, surface tension is unable to render them completely round- instead they tend to have a flat underside. They look more like a string of air-fluid levels.
One of the functions of the large bowel is to absorb water from the faecal content. The faeces should not be able to form an air/fluid level by the time it gets to the splenic flexure. An extensive arrangement of these small air/fluid levels in the large bowel may simply indicate that the patient has diarrhoea.

Normal Large Bowel Distribution
The large bowel (white arrows) can be seen to frame the abdomen. The prominent air-filled ileum (black arrow) occupies a more central location within the peritoneal cavity. These distribution features can be helpful in differentiating large bowel from small bowel.
Normal Variation of Large Bowel Distribution
As with all anatomical features, there is normal variation. This patient's transverse colon (white arrow) dips low into the pelvis. Note the characteristic haustral pattern of the large bowel.


Dilated Sigmoid Colon
The dilated sigmoid colon is often difficult to positively identify. This patient has dilated colon which is sited mid to low abdomen. The maximum diameter is 88mm.
Small bowel rarely dilates to more than 50mm. The position, size and ambiguous wall pattern suggest that this is dilated sigmoid colon.
...if you can't identify the bowel, think sigmoid colon.

The Gastrocolic Ligament
The gastrocolic ligament is the major apron-like part of the greater omentum which attaches the stomach to the transverse colon. Unfortunately, this ligament can vary in length up to 15cm. Despite this variable length, if you can identify the greater curve of the stomach, you can hazard a reasonable approximation of where the transverse colon should be.
This patient has a dilated stomach which has been treated with a naso-gastric tube. The transverse colon can be seen to be following the greater curve of the stomach.

Pneumoperitoneum
This is a post-op supine abdominal image. The large central air-filled structure (white arrow) does not demonstrate any consistent features of large or small bowel anatomy. It is likely to represent a post-op surgical pneumoperitoneum

Summary
Differentiation between small and large bowel visualised on an abdominal plain film can be a perplexing task. In the presence of abnormally dilated bowel, the usual distinguishing features can be lost and confident differentiation may not be possible. Knowledge of the normal features of stomach, small bowel, and large bowel will assist in making an informed differentiation.
.....return to the Applied Radiography page