Imaging Supracondylar Fractures of the Humerus
Supracondylar fractures of the elbow are one of the most common fractures in children. Achieving satisfactory imaging of these fractures can present the trauma radiographer with a significant challenge. In addition to the normal difficulties associated with imaging children, the radiographer must consider that the patient may be in severe pain and may be accompanied by anxious parents. This page considers what you are trying to achieve radiographically in imaging supracondylar fractures and how best to approach the task.
The Lateral Elbow
Lateral Elbow
<a class="external" href="http://www.radiologyassistant.nl/en/4214416a75d87" rel="nofollow" target="_blank"></a>
<a class="external" href="http://www.radiologyassistant.nl/en/4214416a75d87" rel="nofollow" target="_blank">www.radiologyassistant.nl/en/4214416a75d87</a>
<a class="external" href="http://www.radiologyassistant.nl/en/4214416a75d87" rel="nofollow" target="_blank"></a>
<a class="external" href="http://www.radiologyassistant.nl/en/4214416a75d87" rel="nofollow" target="_blank">www.radiologyassistant.nl/en/4214416a75d87</a>The lateral elbow projection, paediatric or adult, is one of the most difficult views in radiography. You tend to become familiar with the appearance of a true lateral elbow but it is not easy to describe. The following positioning points are worthy of mention
- the elbow should be flexed to 90 degrees if possible
- the patient's wrist should be in a lateral position
- The patient's hand should be raised slightly (may need to be lowered in children)
- the patient's humerus should be horizontal
This position is taught as an incorrect lateral elbow radiography position. With the patient's wrist in a PA position, the radius (not the ulna) is in a PA position (think about the elbow).
If you are aiming to demonstrate the distal humerus in a true lateral position to assess: elbow fatpads; the anterior humeral line; and other evidence of supracondylar fracture, this position is acceptable and may even achieve an improved result. This is because, in the younger child, it is more likely that a lowered wrist position will be required to achieve a true lateral elbow position. (see example below)
Important Point of Interest
If you have positioned the patient's wrist in a PA position for both elbow projections, you will have demonstrated the radius in a PA projection only on both views. This is an unacceptable radiographic series for assessment of the radius.
Paediatric Lateral Elbow
<a class="external" href="http://www.radiologyassistant.nl/en/4214416a75d87" rel="nofollow" target="_blank">
</a>
The radiographer has performed 'mixed' views of the forearm. These images are inadequate for assessment of a supracondylar fracture.
image taken from forearm views aboveThe anterior humeral line falls within the anterior third of the capitellum suggesting a supracondylar fracture. The radiographer considered this appearance to be projectional rather than pathological. The lateral projection was repeated.
image taken from forearm views aboveThe question arises as to how to correct the malpositioned lateral elbow- does the patient's hand need to be lowered or raised to rotate the distal humerus into a lateral position? The arrowed structure is the lateral condyle of the humerus and is often demonstrated as a smoothly contoured convex posterior bony contour on both adult and paediatric lateral elbow projection images. This appearance suggested the patient's elbow needed to be raised/hand lowered to rotate the humerus into a more lateral projection. The radiographer repeated the lateral elbow view by raising the patients elbow resulting in an improved lateral elbow position. The anterior humeral line can now be seen to fall within the middle third of the capitellum suggesting no displaced supracondylar fracture is present.
Note that the patient's elbow was raised (not the hand) to correct the malposition.
The Adult Lateral Elbow
This is an acceptable lateral elbow position.
- The elbow is flexed to an approximate right angle (90 degrees)
- The capitellum, medial lip of the trochlea and trochlear notch (the 3 rings) are concentric.
This is not a true lateral elbow position. The positioning error is largely associated with the patient's forearm position. If the patient's hand is lowered minimally, the capitellum (white dotted outline) will move anteriorly and the trochlea (yellow outline) will move posteriorly.
- The elbow is not flexed to 90 degrees
- The 3 rings' are not concentric.
This lateral elbow would probably not be repeated- the decision to repeat this view should be based on a balanced assessment of cost vs benefit.This is not a true lateral elbow position. The positioning error is caused by a failure to position the humerus in a true horizontal position (in addition there is a failure to lower the patient's hand to the correct level). Correct this position by lowering the patient's elbow- this will project the capitellum outline distally and the trochlea outline proximally. The other correction can be achieved by lowering the patient's hand.
- The elbow is not flexed to 90 degrees
- The 3 rings' are not concentric.
This lateral elbow would arguably not be repeated- the decision to repeat this view should be based on a balanced assessment of cost vs benefit.















Minimum AP Dimension
If you have achieved the correct position, the elbow will be flexed to 90 degrees, the patient's wrist will be in the lateral position, and the distal humerus will have a minimum antero-posterior dimension. The distal humerus is wider in its lateral dimension than in its AP dimension. Therefore, if you start with a perfectly lateral elbow, and you rotate it off lateral, the distal humerus it will increase in its AP dimension. In other words, a true lateral elbow will demonstrate the distal humerus at its narrowest.

The Hockey Stick Analogy
The lateral elbow has been likened to a hockey stick shape as shown left. Whilst it is undeniable that this lateral elbow looks hockey stick shaped, this is not a useful aid in assessing lateralness. A lateral elbow can be very "off-lateral" and still retain the hockey stick shape.
The Figure Eight or Hour Glass Sign
Second Attempt 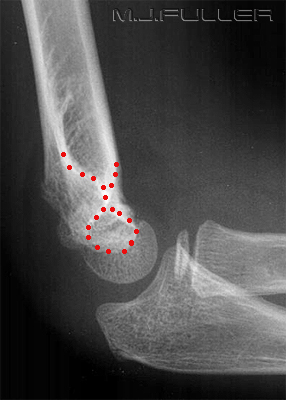
This is the first attempt at a lateral elbow. Note the absence of the figure eight sign. Note also the medial epicondyle ossification centre projected posteriorly. This is the second attempt at the lateral elbow.
The patient's wrist has been raised slightly. This movement has caused the medial epicondylar ossification centre to be partially superimposed over the distal humerus and the radial head to further overlap the ulna. This is logical if you think about the relationship between the anatomical structures.
A better position has been achieved and the
figure eight sign is now evident
Note a subtle supraconylar fractureSecond attempt (same image) with figure eight sign marked Important
The figure eight sign does not indicate a perfectly positioned lateral elbow. However, the absence of the figure eight sign could indicate that the elbow is not lateral, or that the elbow is fractured, or both.




The Supinator Fatpad Sign
The supinator fat pad can be raised or obliterated as a result of bony injury, particularly to the radial head. It is one of those unreliable soft tissue signs, but it is worth examining as a guide to potential bony injury, particularly to the radial head. The supinator fatpad can also be displaced by an elbow joint effusion.
Tip
If you have trouble remembering whether it is the supinator fat pad sign or the pronator fat pad sign, think of a restaurant waiter. Waiters sometime carry soup bowls (ie "soupinator") in their elbows.
..... pronator fat pad at the wrist.... supinator fat pad at the elbow.

Elbow Joint Effusion (sail sign)
<a class="external" href="http://books.google.com.au/books?id=6AXkE4y1678C&pg=PA509&lpg=PA509&dq=radial+head+fractures+incidence+in+adults&source=bl&ots=JRFuoZ23Kh&sig=r6wMfpmEAfwn6_ySqvaTdogcJVk&hl=en&ei=u_FHSvmRIIfU7AOqkZnoAw&sa=X&oi=book_result&ct=result&resnum=9" rel="nofollow" target="_blank">Charles A. Rockwood, Kaye E. Wilkins, James H. Beaty, James R. Kasser</a>
<a class="external" href="http://books.google.com.au/books?id=6AXkE4y1678C&pg=PA509&lpg=PA509&dq=radial+head+fractures+incidence+in+adults&source=bl&ots=JRFuoZ23Kh&sig=r6wMfpmEAfwn6_ySqvaTdogcJVk&hl=en&ei=u_FHSvmRIIfU7AOqkZnoAw&sa=X&oi=book_result&ct=result&resnum=9" rel="nofollow" target="_blank">Rockwood and Wilkins' fractures in children</a>
<a class="external" href="http://books.google.com.au/books?id=6AXkE4y1678C&pg=PA509&lpg=PA509&dq=radial+head+fractures+incidence+in+adults&source=bl&ots=JRFuoZ23Kh&sig=r6wMfpmEAfwn6_ySqvaTdogcJVk&hl=en&ei=u_FHSvmRIIfU7AOqkZnoAw&sa=X&oi=book_result&ct=result&resnum=9" rel="nofollow" target="_blank">Lippincott Williams & Wilkins, 2006</a>The elbow joint is a synovial joint. When an elbow injury occurs and there is intra-articular involvement, there can be an associated elbow joint effusion. As the elbow joint distends with fluid, the adjacent soft tissues can be displaced. The anterior and posterior fat pads are of particular interest to radiographers because they can provide a valuable indicator of intra-articular injury when the elbow fat pads are displaced by an elbow joint effusion. Importantly, evidence of an elbow joint effusion on elbow plain film images does not indicate a definite elbow fracture- it does indicate an elbow joint injury.
An intra-articular elbow fracture can haemorrhage and distend the synovium rapidly.The anterior elbow fat pad can often be seen in a normal lateral elbow as a stripe of radiolucency parallel to the anterior cortex of the distal humerus. A visible anterior fat pad can be a normal finding- a visible posterior fatpad is not a normal finding.
<a class="external" href="http://books.google.com.au/books?id=6AXkE4y1678C&pg=PA509&lpg=PA509&dq=radial+head+fractures+incidence+in+adults&source=bl&ots=JRFuoZ23Kh&sig=r6wMfpmEAfwn6_ySqvaTdogcJVk&hl=en&ei=u_FHSvmRIIfU7AOqkZnoAw&sa=X&oi=book_result&ct=result&resnum=9" rel="nofollow" target="_blank">Charles A. Rockwood, Kaye E. Wilkins, James H. Beaty, James R. Kasser</a>
<a class="external" href="http://books.google.com.au/books?id=6AXkE4y1678C&pg=PA509&lpg=PA509&dq=radial+head+fractures+incidence+in+adults&source=bl&ots=JRFuoZ23Kh&sig=r6wMfpmEAfwn6_ySqvaTdogcJVk&hl=en&ei=u_FHSvmRIIfU7AOqkZnoAw&sa=X&oi=book_result&ct=result&resnum=9" rel="nofollow" target="_blank">Rockwood and Wilkins' fractures in children</a>
<a class="external" href="http://books.google.com.au/books?id=6AXkE4y1678C&pg=PA509&lpg=PA509&dq=radial+head+fractures+incidence+in+adults&source=bl&ots=JRFuoZ23Kh&sig=r6wMfpmEAfwn6_ySqvaTdogcJVk&hl=en&ei=u_FHSvmRIIfU7AOqkZnoAw&sa=X&oi=book_result&ct=result&resnum=9" rel="nofollow" target="_blank">Lippincott Williams & Wilkins, 2006</a>
In the presence of an elbow effusion, the fatpads can be displaced in an appearance that is commonly referred to as a sail sign. When you see a sail sign on a lateral elbow image, consider carefully whether you have adequately demonstrated a related fracture, and if not, whether supplementary views would be worthwhile to determine if a fracture exists. Note also a subtle posterior fatpad sign (left)- this is subtle but important in that it suggests a probability of fracture at about the 90% level.
source: unknownElbow fatpad sign (sail sign) is usually present in patients with supracondylar fractures. The bony injury will usually result in a haemarthrosis. The distal humerus has two fossae- the coronoid fossa accommodates the coronoid process of the ulna on elbow flexion and the olecranon fassa accommodates the olecranon process of the ulna on elbow extension. The coronoid fossa is a shallower fossa than the olecranon fossa- this is why the anterior fat pad can appear as a normal elbow feature and also explains why an anterior fat pad assign can appear without the posterior fat pad sign. ie it takes a larger elbow effusion to displace the posterior fat pad out of the deeper olecranon fossa than the anterior fat pad out of the shallower coronoid fossa.





Anatomy
In a normal elbow, anterior fat pad is nestled in the coranoid fossa. The posterior fat pad occupies the olecranon fossa. The olecranon fossa is larger to accommodate the olecranon, and the coronoid fossa is smaller to accommodate the coronoid. This is consistent with the observation that a larger elbow joint effusion is required to reveal the posterior fat pad. Note that this patient has a visible normal anterior fat pad.
Don't get the coracoid of the shoulder confused with the coronoid of the elbow.In a normal elbow, anterior fat pad is nestled in the coranoid fossa. The posterior fat pad occupies the olecranon fossa. The olecranon fossa is larger to accommodate the olecranon, and the coronoid fossa is smaller to accommodate the coranoid. This is consistent with the observation that a larger elbow joint effusion is required to reveal the posterior fat pad. Note that this patient has a visible normal anterior fat pad.
Don't confuse the coracoid of the shoulder with the coronoid of the elbow.


Normal Anterior Humeral Line Abnormal Anterior Humeral Line The normal alignment lines of the elbow can be a guide both to good positioning and the existence of subtle pathology. The important line for diagnosis of supracondylar fractures is the anterior humeral line.
The anterior humeral line is a line drawn along the anterior cortex of the distal humerus in the lateral view. This line is described as passing through the middle third of the capitellum. (some texts suggest that it should lie at the junction of the middle and anterior third of the capitellum). If it is clearly not in this position, it suggests that the elbow is not lateral or that there is a fracture.
The anterior humeral line will not always divide the anterior and middle thirds of the capitellum. Radiographic malpositioning, measurement error, and individual anatomical variation will see this line fall within region 2 in most patients. If the anterior humeral line falls within region 2 (see left) the position does not support a displaced supracondylar fracture.Region 3 is the danger zone- most supracondylar fractures involve posterior displacement of the distal fragment. As the distal fragment (capitellum) is displaced posteriorly, the anterior humeral line will move into region 3.



Comparison Views
Routine comparison views are rarely warranted in radiography and the elbow is no exception. In the words of John Harris et al
"Routinely obtaining even anteroposterior and lateral radiographs of the opposite elbow (or other appendicular joint for that matter) 'for comparison' fails the standard of current radiological care." John Harris et al (The Radiology of Emergency Medicine, 3rd Ed, Williams and Wilkins, 1993, p 336)
There is an argument for comparison views in certain circumstances. The argument for not performing comparison views is that if you understand normal anatomy, comparison views are unnecessary. The junior doctor in the Emergency Department at 0300hrs will provide the counter-argument that he/she is not familiar with nuances of paediatric bony anatomy and may require comparison views in order to avoid misdiagnosis.
The Gartland Classification of Supracondylar Fractures
Gartland Type I Supracondylar Fracture Gartland Type II Supracondylar Fracture Gartland Type III Supracondylar Fracture


Supracondylar or Intercondylar?
We tend to label all transverse fractures of the distal humerus as supracondylar fractures even when they are intercondylar. John Harris et al notes the following
"The most common fracture of the paediatric elbow is the supracondylar or transcondylar fracture. Because the distinction is frequently only a matter of millimetres, because an oblique fracture often includes both transcondylar and supracondylar regions, and because injury to the brachial neurovascular trunk is common to posteriorly displaced supracondylar and transcondylar fractures, it seems reasonable to consider all fractures in this region as supracondylar for radiographic diagnostic purposes" John Harris et al (The Radiology of Emergency Medicine, 3rd Ed, Williams and Wilkins, 1993, pp 351,352)
The CRITOL Rule
The appearances of the ossification centres of the elbow frequently causes confusion. The CRITOL rule is a memory aid that lists the order of appearance of the elbow ossification centres
The order of appearance of the elbow ossification centres is as follows
1. Capitellum
2. Radial Head
3. Internal (medial epicondyle)
4. Trochlea
5. Olecranon
6. Lateral Epicondyle
The capitellum contributes to the growth of the humerus and is therefore considered an epiphysis. The other ossifications centres are called traction epiphyses or apophysis.
Some Important Notes about the CRITOL Rule
- It is not uncommon for the ossification centres to appear out of order
- The ages at which the ossification centres appear are approximate only. Different texts will suggests different ages
- The trochlea often appears fragmented- this is normal
- the "I" in CRITOL refers to the medial epicondylar ossification centre ("I" for internal)

Clinical Signs of Supracondylar Fracture
- most common elbow fracture in children
- pain and swelling
- decreased range of movement
- deformity
The Characteristic Anterior Cortical Defect
Supracondylar fractures in children often demonstrate acharacteristic distal humeral anterior cortical defect. The following cases provide examples of ths defect.




Case 1
This 5 year old boy presented to the Emergency Department after falling onto an outstretched hand. He presented with a severely swollen and painful elbow. He was referred for imaging of his elbow.
Case 2
This is a lateral view image of the boy's elbow. There is rotation of the distal fragment relative to the proximal fragment. This is a Gartland type III supracondylar fracture. The AP view horizontal ray image demonstrates medial displacement and rotation of the distal fragment. Comment
A child with severely swollen and anatomically distorted elbow should be assumed to have an unstable fracture/dislocation until proven otherwise. The AP and lateral views should be performed without moving the patient's elbow to ensure that there is no additional soft tissue damage during the X-ray examination.
Gartland type III supracondylar fractures of the elbow require timely reduction to minimise the chances of vascular and nerve damage. The radiographer should advise the referring doctor of a Gartland type III fracture immediately.

This 4 year old girl presented for radiography of her right elbow following referral from orthopaedic clinic. She presented with her right arm in an above-elbow plaster backslab cast.
The initial lateral view image was not a true lateral elbow position and was considered worthy of repeating. You cannot accurately assess the degree of posterior angulation of the distal fragment on this view- assessment of this angular displacement was an important reason for referring the patient for the X-ray examination. The repeat lateral elbow is a considerable improvement on the first attempt. The hour-glass sign is clearly evident. The anterior humeral line does not lie within the middle third of the capitellum indicating some residual dorsal angulation of the distal fragment The anterior humeral line falls within the anterior third of the capitellum suggesting posterior displacement/angulation of the distal fragment. The AP elbow projection presents technical difficulties. It is evident that conventional AP elbow radiographic technique cannot be applied. The distal humerus is the area of interest and imaging should be undertaken with this in mind. The radiographer has positioned the patient's humerus in the AP position on the IR. The distorted semi-axial image of the forearm is of incidental note- this is not the anatomy of interest. It is sometimes necessary to angle the beam towards the patient's hand to ensure successful visualisation of the supracondylar anatomy (some text recommend routine 10 degree angulation).
An alternate approach is to perform an axial view of the elbow. This is more likely to be successful when the elbow is fixed in a high level of flexion.
The low contrast image of the bony anatomy is a legacy of thick plaster and thin paediatric bone. High resolution and edge enhancement may detract from the image (improved visualisation of the plaster rather than the bone).Comment
Follow-up imaging of paediatric supracondylar fractures requires flexibility in technique. Consideration should be given to
- sitting the child on the parent's knee
- performing the imaging with the patient in the standing position
- lying the patient down on the X-ray table




Case 3
This 80 year old man presented to the Emergency Department following an unwitnessed fall. His elbow was swollen and painful. He was referred for elbow radiography.
This is an AP elbow image with the elbow in flexion. The position is biased towards demonstration of the radius and ulna by positioning the forearm in contact with the image receptor.
There is a clearly demonstrated supracondylar/intercondylar fracture of the humerus.This an AP elbow image with the humerus in contact with the image receptor. This approach is arguably better than the single view AP which tends to produce compromised imaging of both the humerus and radius/ulna.
The AP elbow image positioned for demonstration of the humerus affords a different impression of the degree of lateral displacement of the distal fragment.The lateral elbow image demonstrates anterior displacement of the distal fragment. A 45 degree radial head view was performed. No displaced radial head fracture is demonstrated. Comment
Supracondylar fractures of the distal humerus are associated with paediatric trauma but are occasionally seen in the adult population. The radial head view was arguably unnecessary. In cases of obvious bony deformity it is prudent to perform a single exposure scout radiographic examination in order to establish the nature of the deformity. This provides information on which to base the subsequent plain film imaging.




Case 4
This 4 year old girl presented to the Emergency Department following a fall onto an outstretched hand (FOOSH). Her right elbow was swollen and painful. She was referred for elbow radiography.
The AP elbow image suggests a possible supracondylar fracture line (not entirely convincing from this single image). The lateral elbow image demonstrates anterior and posterior fat pad signs.
The anterior humeral line is normal
There is a very small cortical irregularity of the distal humerus (arrowed) which may represent a supracondylar fracture.
There is also a lucent line seen in the posterior aspect of the distal humerus which may represent an undisplaced supracondylar fracture (not marked).The radial head view demonstrates a cortical irregularity posteriorly with an associated lucency. This may represent an undisplaced supracondylar fracture. Comment
This case demonstrates a frequent finding in acute paediatric elbow imaging- the subtle or equivocal fracture. Good quality imaging will improve the likelihood of a correct diagnosis. The referring doctor will arrive at a likely diagnosis in these types of cases based on a balanced consideration of
- the age of the child
- the mechanism of injury
- the clinical signs
- the radiographic evidence.
It is likely that this child would have appropriate immobilisation of the elbow, pain relief, and a follow-up appointment at orthopaedic clinic.
Whilst a radial head fracture would fit with the clinical signs, a child is more likely to have sustained a supracondylar fracture with this history. The radial head view was arguably an unnecessary inclusion in the initial radiographic series.


Case 5
This 7 year old girl presented to the Emergency Department after an unwitnessed fall. She was referred for radiography of her left elbow.
The axial elbow view was performed in lieu of the conventional AP view. The lateral view image confirms the supracondylar fracture. This is a typical Gartland type I supracondylar fracture. The cortical defects with this type of fracture in children tend to be sited as shown in this case. They are often subtle. A close examination of the anterior humeral line can be helpful. The anterior humeral line can be seen to lie within the anterior third of the capitellum suggesting a posterior angulated supracondylar fracture.


Case 5
This 10 year old boy presented to the Emergency Department after falling onto an outstretched hand. He was very tender around the left elbow. He was referred for radiography of his left elbow.
The AP elbow image is unremarkable The lateral view image demonstrates anterior and posterior fatpad signs (white arrows). There are a few cortical defects of the distal humerus anteriorly (black arrows) which may represent a supracondylar fracture. The anterior humeral line can be seen to lie within the middle third of the capitellum suggesting no displaced fracture.


Comment
This case is typical of a Gartland I supracondylar fracture . You will often have an age group, a mechanism of injury, soft tissue signs, and a subtle cortical defect on which to base a diagnosis.
Case 6
This 6 year old boy presented to the Emergency Department with a painful left elbow after falling of play equipment. He was examined and referred for left elbow radiography.
There is evidence of anterior and posterior fatpad signs.
There is evidence of a minimally displaced supracondylar fractureThe anterior humeral line does not divide the capitellum into thirds suggesting posterior displacement of the distal fracture fragment. The AP projection image demonstrates the fracture line clearly, particularly through the medial condyle.



...back to the Wikiradiography home page
...back to the Applied Radiography home page