What is the Value of the Lateral Chest Projection?
Some institutions (or even countries/continents) perform lateral chest radiography as a routine view whilst others almost never do. Is the lateral chest X-ray useful and, if so, is it useful enough to warrant its inclusion as a routine view? Has the cost/benefit equation changed with the introduction of digital imaging? Some radiologists have argued that the lateral chest view is never required- all pathology can be seen on the AP/PA.... but these radiologists are usually not around at 0300hrs in the Emergency Department when the image interpretation/treatment decision could be taking place.
You could argue that the lateral chest projection is required on the basis of selected case studies where it can be shown to reveal or clarify significant chest pathology. But wouldn't this be an argument for performing chest radiography as a screening tool on asymptomatic patients? (if you randomly perform chest radiography on the asymptomatic population you will find significant pathology)
Would the health care resources spent on lateral chest radiography provide a better yield if spent elsewhere?
If you are only performing AP/PA chest radiography, could an argument be made for more bedside chest radiography in the wards?
The Cases
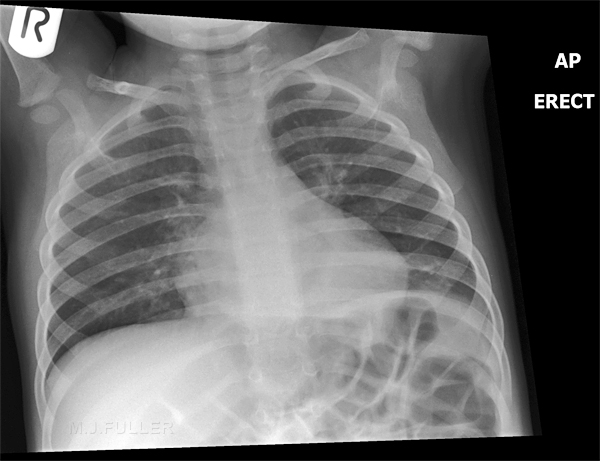
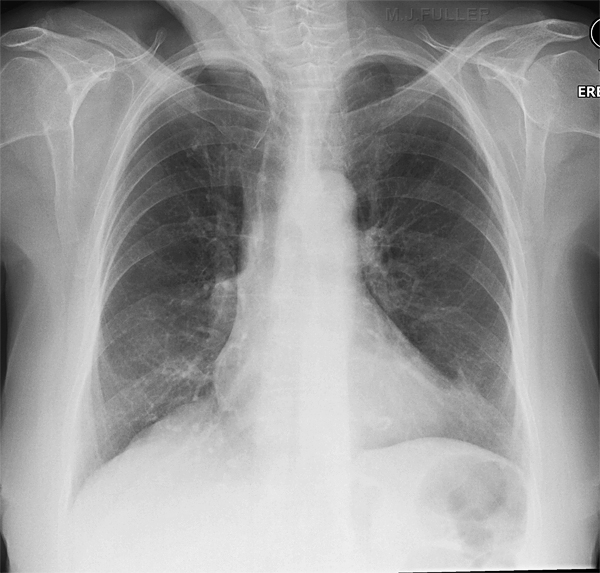
If you are one of those people that advocate a "PA only" approach to chest radiography, consider the cases below. Each case has had AP/PA and lateral views of the chest. Can you confidently identify the pathology without the aid of the lateral projection?
Some cases are quite easy in terms of image interpretation and some are difficult
Case 1
Answer
Case 2
Answer
Case 3
Answer
Case 4
Case 5
Answer 5
Case 6
answer
Case 7
answer
Case 8
Answer
Case 9
Answer
Case 10
Answer
Case 11
Case 12
Answer
Case 13
Answer
Case 14
Answer
Case 15
Answer
Case 16
Case 17
Case 18



The Exceptions
Not every patient who is referred for chest radiography should be subject to a lateral view. B Golberg refers with great wit to the "fish and Chips" lateral...
I have written mainly... about what I classify as the
"fish and chips" lateral view-a request made purely from habit
or conditioned reflex. In the same week as I received the annotated
form mentioned in the first paragraph a casualty officer,
on his first day at the hospital, requestedposteroanterior and
lateral views " ? pneumothorax."
An experienced radiographer did the correct examination-namely, views in inspiration and expiration, only to receive patient and form back immediately
with the insistence that a lateral view be done. Such a view is certain to be useless if he really was looking for a pneumothorax. If there was something else on his mind it was certainly not on the request form.<a class="external" href="http://www.pubmedcentral.nih.gov/picrender.fcgi?artid=1601086&blobtype=pdf" rel="nofollow" target="_blank">B Golberg, BRITISH MEDICAL JOURNAL 29 MARCH 1980, p 909</a>
Links
- <a class="external" href="http://education.thoracicrad.org/2007/BTB/735/player.html" rel="nofollow" target="_blank">http://education.thoracicrad.org/2007/BTB/735/player.html</a>
Discussion
I am hoping that there will be some attempt(s) to interpret these images without the lateral view. You can post your comments using the "post a new thread" link at the bottom of this page. Once a few brave souls have had a go, I will post the lateral chest images.
I have very little doubt that an expert in chest image interpretation will correctly identify the pathologies on this page without the benefit of the lateral chest image. This is arguably not the point- the person who views the image and acts upon the findings needs to be furnished with images that allow him/her to arrive at the correct diagnosis. It is often the case that pathologies that are sited behind the heart shadow or below the diaphragm are easier to appreciate with the aid of a lateral image. Are you left wondering how many chest pathologies you have missed over the years?
back to the Applied Radiography home page