The Supine Pneumothorax
Radiographers quickly develop the image interpretation skills required to identify a pneumothorax demonstrated on an erect chest X-ray image. The identification of a pneumothorax on a supine chest X-ray image is a more difficult task. The supine pneumothorax can be undetectable or the signs may be very subtle. This page considers some of the pattern recognition skills and radiographic techniques required to identify a supine pneumothorax.
Definition of Terms
Erect vs Supine PneumothoraxPneumothorax
Pneumothorax refers to air in the pleural space. The pleural space is normally a potential space.
Pleural Space
The potential space between the parietal and visceral pleural surfaces
What to Look forWhy should the plain film appearances of pneumothorax be different for erect and supine images? The answer has everything to do with gravity. The lung affected by the pneumothorax is partially free to move under the effects of gravity because it is not limited by the normal constraints of the uncompromised pleural space. A lung which has been compromised by pneumothorax will tend to fall into the most dependent position in the thoracic cavity.
Erect Position
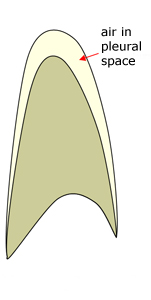
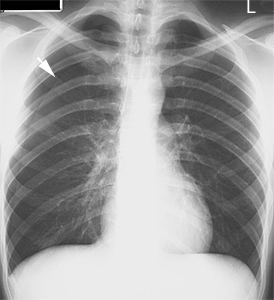
In the erect position the lung will tend to fall towards the diaphragm. This is why the pneumothorax is often most evident at the lung apex (arrow). Note that the lung is attached at the hilum and will therefore tend to collapse inferiorly and medially in the erect position.
In the supine position the lung will tend to fall to the posterior chest wall. The pneumothorax will usually be evident near the diaphragm first.



As the diagram above suggests, in the supine position, air in the pleural space will tend to collect anteriorly and inferiorly. Tocino (1) describes the situation as follows
"In the supine position, the anteromedial space becomes the least dependent
pleural recess. Air in this space may reveal the earliest and, often,
most subtle radiographic signs of pneumothorax. As the volume of air in-
increases, signs of pneumothorax will extend into the subpulmonic space and
then into the apicolateral space.
The anteromedial space is divided by the hilar structures into superior
and inferior compartments. Initially, air will accumulate preferentially in one
of these compartments. Air in the superior anteromedial space accounts for
the sharp delineation of mediastinal contours ...... . In fact, air interposed
between abnormal lung parenchyma and the mediastinal structures
(absence of the silhouette sign) should raise suspicion of pneumomediastinum
or pneumothorax."
Radiographic TechniqueSigns of Supine Pneumothorax
Sign Description 1 Etched Diaphragm Diaphragm contrasted with air in pleural space 2 Etched Mediastinum Mediastinum (heart border) outlined with air in the pleural space 3 Deep Sulcus Sign Abnormally prominent/deep costophrenic angle 4. Visible Visceral Pleura Most often seen as a doublediaphragm-like appearance 5. Mediastinal shift As in the erect position, mediastinal shift may indicate the presence of a pneumothorax under tension 6. Uneven Lung Density Affected lung may appear abnormally translucent. Abnormal lung may also appear abnormally opaque in hydropneumothorax from veiling density 7. Absent Lung Markings This will usually occur in the presence of other signs
1. The Etched Diaphragm and Etched Mediastinum SignsThe supine pneumothorax is best demonstrated on full expiration. A caudally angled image centred on the diaphragm may be of some assistance in the presence of a subpulmonic pneumothorax. A supine cross-table lateral chest may provide further evidence of pneumothorax by displaying air accumulated anteriorly in the pleural space. An apical lordotic view may also help to demonstrate a pneumothorax but is more likely to be of assistance with the patient in the erect position.
If the patient is able to be imaged in the erect position this will clearly be advantageous.
| | This is a supine chest X-ray image on a patient in the intensive care unit. The right hemidiaphragm appears highly contrasted/delineated against the right lung. The reason for this is that there is a right pneumothorax and the right hemidiaphragm is delineated by air in the pleural space rather than lung. This is sometime referred to as etched diaphragm. Occasionally, this will be the only evidence of supine pneumothorax. Notice that there are no lung structures visualised through the right hemi-diaphragm. Compare this patient's right hemidiaphragm with the image below. There is mediastinal shift to the left. The right lung edge is visible |
| | There are a variety of signs of pneumothorax on this image. Note that the left heart border appears too contrasty or delineated. Compare it with the right heart border. This is an example of etched mediastinum. The high contrast left heart border is caused by the change in the adjacent structure- on the right, the heart border is in contact with lung, while on the left, the heart border is in contact with air in the pleural space. |


| This is the first chest X-ray taken on a newborn premature baby. Arterial and venous umbilical catheters are demonstrated. There is a general impression of lucency of the right lung compared to the left. There is evidence of right pneumothorax- the right lung margin is seen at the level of the right scapula. Further evidence of right pneumothorax is evident from etched diaphragm and etched right heart border. This is a subtle sign that is worth learning because it may be the only sign of pneumothorax in a supine technique chest X-ray image. If you look critically at the right diaphragm and heart border you will see subtle evidence that they are more contrasty than on the left. The right heart border and diaphragm appear more delineated because they are bordered by air in the pleural space rather than lung. This could be considered a reverse silhouette sign. Radiographers who have developed their image interpretation skills to a level where they are able to detect etched diaphragm and etched mediastinum could consider themselves to have reached an advanced level. |

| | This patient also has an etched right hemidiaphragm. This is considerably more subtle than the previous example. There is often just an impression that one of the hemidiaphragms looks too well delineated. In such a case you would look for other supporting evidence of pneumothorax. In this case, we will ignore the UWSD for a moment. The other supporting evidence in this film is as follows
... and of course, UWSD |

| |  |
| The dotted line is the medial margin of the collapsed lung outlined by air in the pleural space Source: <a class="external" href="http://www.mypacs.net/cases/SUPINE-PNEUMOTHORAX-ON-DAY-1-CXR-11464797.html" rel="nofollow" target="_blank">http://www.mypacs.net/cases/SUPINE-PNEUMOTHORAX-ON-DAY-1-CXR-11464797.htm</a>l |

2. Deep Sulcus Sign
| | The right costophrenic angle can be seen to be very low. This is known as deep sulcus sign. This is usually accompanied by an unusually translucent appearance to the subdiaphragmatic anatomy |
3. The Other Views
| | It's surprising how often a pneumothorax is visible on other views, particularly the AP cervical spine and AP shoulder views. This patient has a right sided pneumothorax visible on this AP cervical spine view. Note the edge of the lung (arrowed) and the lack of lung markings in the right second intercostal space compared with the contralateral side. |

4. False Pneumothorax
| | A false pneumothorax is most commonly caused by a skinfold. This is not a trivial finding. If a skin fold is misinterpreted as a pneumothorax the patient may have an Underwater Sealed Drain (UWSD) inserted.... and then they will have a pneumothorax. This appearance will be seen most commonly in supine and erect bedside chest radiography where the patient is in direct contact with the cassette/IR. It will also be more common in the elderly who are more likely to have loose skin |

5. Tension Pneumothorax
| | This is a supine chest image on a patient who was involved in a motor vehicle accident (MVA). There is a large right pneumothorax which is under tension. The tension has resulted in considerable mediastinal shift. There is a severe deep sulcus sign. Tension pneumothorax results from a ball valve effect which causes air entry into the pleural space with reduced or no air out of the pleural space. Tension pneumothorax is a life-threatening condition. |

6. Mediastinal Shift
| | The most obvious sign of pneumothorax on this image is mediastinal shift to the right. Also note
|
7. Visible Visceral Pleura
| | One of the more obvious signs of pneumothorax on an erect AP/PA chest image is the edge of the lung. Normally the visceral pleura is not visible because it is in close contact with the parietal pleura- the pleural space is normally a potential space. This patient has a right sided pneumothorax. The arrowed structure is the lung edge. This is a subpulmonary pneumothorax. |
8. Uneven Lung Opacity
| | The left lung appears more opaque than the right lung. The increased translucency of the right lung is caused by the right pneumothorax. Care must be taken in explaining uneven lung density. There may be other causes and complicating pathologies. The pneumothorax lung may also appear hyperdense because of a veiling opacity caused by blood in the pleural space. |
Supine Pneumothorax sizing
Pneumothorax sizing would not normally be attempted on a supine image. A study published in Radiology by Byung Gil Choi (2) aimed to correlate pneumothorax size measured on a supine image with that measured on an erect image. The researchers derived a new nomogram for supine chest radiography as follows
Pneumothorax Nomogram (2)
Average Interpleural Distance
Corresponding Pneumothorax Size
measured on
Erect PA Image
Corresponding Pneumothorax Size
measured on
Supine AP Image



If you are not familiar with sizing a pneumothorax using the average interpleural distance, there should be plenty of material on <a class="external" href="http://www.google.com" rel="nofollow" target="_blank">google</a>. Note that the average interpleural distance method has been superseded by a new method. The new method is based on CT volume measurements and is more accurate than the previously used method. An Australian Radiographer has written a javascript program which can be downloaded onto your computer and used for accurate measurement of pneumothorax on erect chest images.... downloadable javascript to come!?
Discussion
A pneumothorax is a serious finding and should be reported by the radiographer to the referring doctor as soon as possible (check your department protocol). Radiologists will be very familiar with the signs of supine pneumothorax whereas most clinicians wont- the assistance of the radiographer in identifying supine pneumothorax can be very helpful. The out-of-hours situation is where the radiographer's image interpretation skills are most likely to be utilised.
Summary
The supine pneumothorax is more difficult to detect than the same sized pneumothorax imaged in the erect position. Knowing the signs of supine pneumothorax will assist you to look in the right places
References
| 1 | Ilrena M. Tocino, M.D. Pneumothorax in the Supine Patient: Radiographic Anatomy. Radiographics Tocino 5 (4): 557. <a class="external" href="http://radiographics.rsnajnls.org/cgi/content/abstract/5/4/557" rel="nofollow" target="_blank">http://radiographics.rsnajnls.org/cgi/content/abstract/5/4/557 </a>. |
| 2. | Byung Gil Choi, MD. Seog Hee Park, MD. Eun Hee Yun, MD. Kyung Ok Chae, MD. Kyung Sub Shinn, MD Pneumothorax Size:Correlation of Supine Anteroposterior with Erect Posteroanterior Chest Radiographs. Radiology 1998; 209:567-569. <a class="external" href="http://radiology.rsnajnls.org/cgi/reprint/209/2/567" rel="nofollow" target="_blank">http://radiology.rsnajnls.org/cgi/reprint/209/2/567</a> |
Further Reading
| 1 | ANDREW R C CUMMIN, MICHAEL J SMITH, ALAN G WILSON, Pneumothorax in the supine patient. BRITISH MEDICAL JOURNAL VOLUME 295 5 SEPTEMBER 1987 <a class="external" href="http://www.pubmedcentral.nih.gov/picrender.fcgi?artid=1248755&blobtype=pdf" rel="nofollow" target="_blank">http://www.pubmedcentral.nih.gov/picrender.fcgi?artid=1248755&blobtype=pdf</a> |
| 2. | Fred M. H. Ziter, Jr.1 Jack L. Westcott. Supine Subpulmonary Pneumothorax . AJR 137:699-70i, October 1981<a class="external" href="http://www.ajronline.org/cgi/reprint/137/4/699" rel="nofollow" target="_blank">http://www.ajronline.org/cgi/reprint/137/4/699</a> |
... back to the Applied Radiography home pgae