The Fissures of the Lung
If you are intent on learning plain film chest pathology, and in particular patterns of collapse and consolidation, you must learn the lobar anatomy and fissures of the lungs first.
Right Lung
The right lung has 3 lobes and two fissures
Lobes
Right Upper Lobe (RUL)
Right Middle Lobe (RML)
Right Lower Lobe (RLL)
FissuresMajor Fissure (aka oblique fissure)
minor fissure (horizontal fissure)The lobes of the lung are further divided into segments. If you are a high achiever, you could learn the segments of the lobes. This can be useful when interpreting consolidation patterns on plain film chest X-ray images- involvement of different segments of a lobe will produce different patterns of consolidation.
The Left Lung

The left Lung is Comprised of two lobes which are divided by one fissure
LobesLeft Upper Lobe (LUL)
Left Lower Lobe (LLL)
Fissures
Major Fissure

Normal Lung Fissures
<a class="external" href="http://books.google.com.au/books?id=Bif0zpmEWtAC" rel="nofollow" target="_blank">
</a>The horizontal fissure of the right lung is the only lung fissure that is normally demonstrated on a PA/AP chest plain film image. The horizontal fissure is evident on PA CXR in about 45% of cases.
The right oblique fissure is more oblique that the left- the left oblique fissure is more vertical probably due to the mass of the heart on the left.
<a class="external" href="http://books.google.com.au/books?id=Bif0zpmEWtAC" rel="nofollow" target="_blank">By Fred W. Wright Radiology of the Chest and Related Conditions: Together with an Extensive Illustrative Collection of Radiographs CRC Press, 2002</a>
- The right and left oblique fissures are somewhat variable in their position- the right oblique fissure can sometimes be positively identified on the lateral image by the horizontal fissure which will stop at the right oblique fissure

Why is the Horizontal Fissure not always Seen on PA/AP Chest Images?
There are probably three common relevant factors.
1. The first is that there is variability in the orientation of the horizontal fissure between individuals. Of particular relevance is the variability of the horizontal fissures horizontalness.
2. Secondly, and possibly more importantly, patients are not always perfectly erect for PA/AP chest radiography. For example, apart from normal random variation in the way patients stand, patients with large protruding stomachs will tend to lean forward for erect PA chest radiography.
3. A third factor is the presence of disease which either pushes or pulls the fissure (i.e. RML collapse).


Pathology Revealing a Fissure?
The example above demonstrates a pathology (RML collapse) causing the horizontal fissure to be hidden on the PA view. The reverse is also true- a pathology can reveal a lung fissure that is nomally hidden.
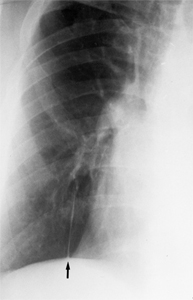
This is a patient with RLL collapse. The PA view demonstrates what looks like a depressed horizontal fissure (arrowed). The lateral image reveals that this is in fact the oblique fissure which has been pulled into an abnormal position by the RLL collapse

What Shape are the Lung Fissures?
source: unknown
- The lung fissures are commonly demonstrated graphically as lines. They are infact a more complex shape and could be drawn more accurately as slightly propeller shaped.
.
- May occasionaly appear as two lines reflecting curve/step-off

Accessory Fissures of the Lungs?
<a class="external" href="http://books.google.com.au/books?id=Bif0zpmEWtAC" rel="nofollow" target="_blank">
</a>Right inferior accessory fissure (arrowed)
Runs in an AP plane (as does the azygous fissure)Usually slightly higher than the right sided horizontal fissure Occcurs in about 4% of the population May incline superiorly laterally
(NOTE HERE ARE A NUMBER OF PATHOLOGICAL APPEARANCES ON THIS IMAGE)Azygous fissure is formed by the anomalous development of the azygous vein The vein migrates through the RUL dragging parietal and visceral pleura with it Azygous fissure (white arrow) and azygous vein (black arrow)




Juxta-phrenic Peak
<a class="external" href="http://www.ajronline.org/cgi/reprint/177/4/869.pdf" rel="nofollow" target="_blank">Eli Konen et al, Prevalence of the Juxtaphrenic Peak After Upper Lobectomy,
AJR:177, October 2001</a>A peak-like shadow along the medial aspect of the right hemidiaphragm is evident in some cases and is referred to as a "juxta-phrenic peak." This finding is more common in left upper lobe collapse, however. The formation of the peak is thought to be related to traction on the basal pleura by the inferior pulmonary ligament. It has also been ascribed to upward retraction of the inferior accessory fissure or an intrapulmonary septum associated with the pulmonary ligament [9]. In severe cases the RUL becomes pancaked against the lung apex or upper mediastinum and can be mistaken for apical pleural thickening. <a class="external" href="http://www.auntminnie.com/index.asp?sec=ser&sub=def&pag=dis&ItemID=53572" rel="nofollow" target="_blank">Scott Williams, Aunt Minnie, April 3, 2002</a>


Right Inferior Accessory Fissure
Right inferior accessory fissure in an 88 year old male who presented to the ED following fall onto his right shoulder.
