Notes on Chest Radiography
<embed allowfullscreen="true" height="350" src="http://widget.wetpaintserv.us/wiki/wikiradiography/widget/youtubevideo/819bedc8891906c19d0bd447c58f0e7e001ec27b" type="application/x-shockwave-flash" width="425" wmode="transparent"/> <embed allowfullscreen="true" height="350" src="http://widget.wetpaintserv.us/wiki/wikiradiography/widget/youtubevideo/a693da619c436ef8be614d64364cda5a00f1ba78" type="application/x-shockwave-flash" width="425" wmode="transparent"/>
1. Chest Radiography of the Kyphotic Patient
2. Bedside Chest Radiography of the Morbidly Obese Patient

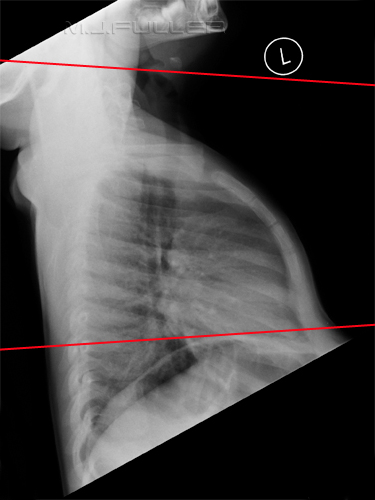
This is a lateral chest image taken on a patient with a moderately severe thoracic kyphosis. A triangular positioning sponge has been placed behind the patient. Note that the patient's chest is angled forward considerably and this position is exacerbated the patient's thoracic kyphosis. The radiographer has, by force of habit, angled the X-ray tube caudally for the AP sitting projection. This is a positioning trap in bedside radiography of kyphotic patients. The result is extreme foreshortening of the chest. Even the use of a horizontal ray would have resulted in significant foreshortening of the lung fields (see the lateral image).



This is an AP sitting bedside chest image of a morbidly obese patient. Whilst largely displaying the chest anatomy, it is lacking in contrast and anatomical structures posterior to the heart are not demonstrated clearly. The technique is non-grid and the exposure factors employed were 95kVp and 6 mAS This is the same patient who has undergone bedside chest radiography the next day. The patient is in the AP sitting position . The radiographer has used an 8:1 ratio stationary grid in the portrait orientation. The risk of grid cut-off is reduced when the grid lines are orientated vertically. The exposure used was 110kVp and 10mAS. Whilst the exposure used is considerably larger than the non-grid technique of the previous day, the results are considerably improved. The disadvantage with this technique, as demonstrated in this case, is that the portrait cassette /grid orientation increases the risk of non-demonstration of the lateral aspects of the chest. ("cutting the sides off" in radiographer parlance). One solution to this problem is to use a 35 x 43 cm grid with the grid lines orientated transversely.
Whether the additional radiation dose to the patient associated with the use of a grid technique is warranted may be a difficult judgement, but should be made "on balance" taking into consideration all of the relevant variables (clinical situation, likely increase in patient dose, diagnostic benefits etc).
A study published in the BJR <a class="external" href="http://bjr.birjournals.org/cgi/reprint/73/873/963" rel="nofollow" target="_blank">(1)</a> concluded that a grid technique was not warranted when using digital selenium radiography. This study did not however consider bedside radiography in morbidly obese patients.
Another study found that it was better to use a solid copper sheet faced cassette to absorb scatter radiation <a class="external" href="http://www.nv-med.com/jsrt/contents/abstract.php?bn=20015704&no=2" rel="nofollow" target="_blank">(2).</a>
Yet another study concluded that with PA chest radiography a 5 to 10 inch airgap would produce similar effects to a stationary grid.<a class="external" href="http://www.ajronline.org/cgi/content/abstract/122/1/109" rel="nofollow" target="_blank">(3)</a>
See also <a class="external" href="http://bloggingradiography.blogspot.com/2008/01/to-grid-or-not-to-grid.html" rel="nofollow" target="_blank">Jeremy Enfinger's</a> excellent website for discussion on this subject, particularly his suggestion of using a short dimension grid.


3. Lateral Chest Arm Position 1
4. Lateral Chest Arm Position 2a
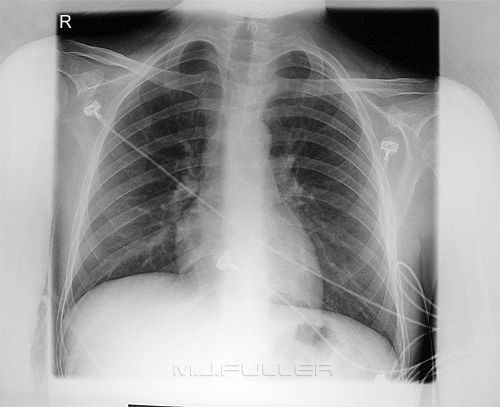
This patient has a right upper lobe (RUL) consolidation. There is abnormal opacity demonstrated above the horizontal fissure of the right lung and an air bronchogram is visible. The lateral chest projection demonstrates the RUL consolidation, but the appearance is complicated by the soft tissues of both arms. The preferred position is to cross the arms across the patient's head (I ask the patient's to "grab opposite elbows") rather than the "hands on head, elbows forward" position.
Benjamin Felson (<a class="external" href="http://www.amazon.com/Chest-Roentgenology-Benjamin-Felson/dp/0721635911/ref=sr_1_2?ie=UTF8&s=books&qid=1252240078&sr=1-2" rel="nofollow" target="_blank">Chest Roentgenology, W.B. Saunders, 1973, p11</a>) notes that "... to delineate the anterior mediastinum, it s better to obtain the lateral view with the arms and shoulder drawn back (military style) rather than extended forward.



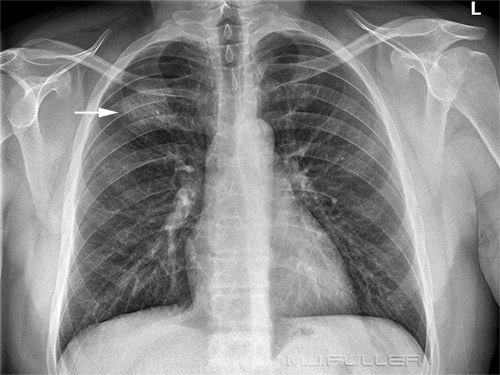
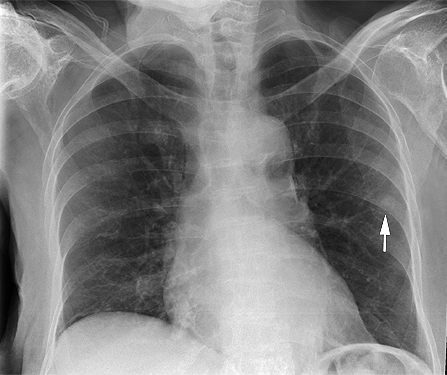
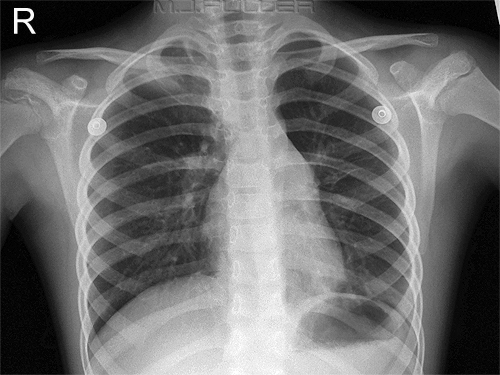
This 32 year old male patient has an abnormal opacity in the RUL. Whilst there are many possible causes of this upper lobe opacity, a round pneumonia or a malignant lesion would be considered.
Note also that the lesion is not partially obscured by the patient's right scapula. The patient's shoulders have been rolled well forward resulting in lung fields unobscured by the scapulae.The radiographer has crossed the patient's arms across his head affording an advantageous view of the lesion without the overlying soft tissues of the patient's arms.



4. Lateral Chest Arm Position 2b
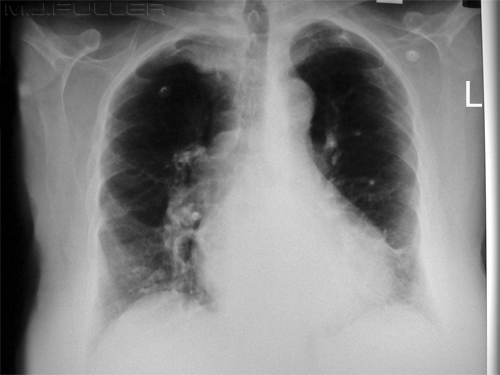
There is abnormal opacity within the RUL abutting the horizontal fissure. The horizontal fissure is slightly bowed and elevated suggesting minor collapse of the RUL associated with the consolidation. The consolidation abuts the horizontal fissure suggesting that the anterior segment of the RUL is involved. The consolidation is likely to be within the anterior segment of the RUL. The arms forward technique has resulted in superimposed soft tissue from both arms largely obscuring the area of interest.


5. Chest Radiography of the Wheelchair-bound Patient

This is a wheelchair-bound morbidly obese patient who was referred for chest radiography. The lateral projection was undertaken first. The patient was leaned forward and a triangular sponge was inserted behind the patient's back. This movement ensured that the patient's anatomy was not superimposed over the metalwork of the wheelchair. The radiographer decided to perform an AP chest technique with the patient in situ in the wheelchair. The triangular sponge was removed from behind the patient's back and the wheelchair was backed up to the upright bucky. The method was simple and effective. This technique benefits from a wheelchair material that is radiolucent. The handles of the wheelchair enforce a compulsory airgap technique.


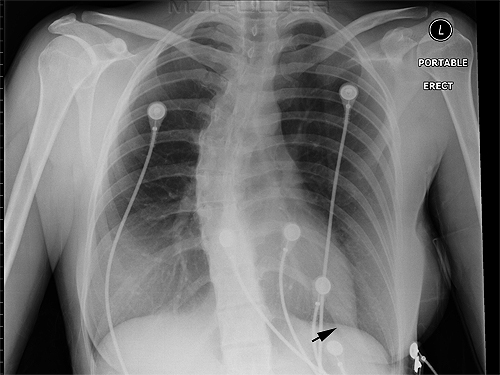
This is a similarly wheelchair-bound. The patient was highly immobile and somewhat slumped into the wheelchair. The radiographer placed a wedge shaped sponge behind the patient back to ensure the patient chest was clear of the wheel-chair's metal frame. The arms of the wheelchair could not be removed. They were considered to not obstruct the lung fields and so were left in-situ. The radiographer decided to perform an AP chest technique with the patient in situ in the wheelchair to good effect. The material of the wheelchair has caused an artifact on the image (arrowed). Despite the associated artifact, on balance, this was considered to be the best available technique at the radiographer's disposal.


This is patient wheelchair-bound. The patient remained in the wheelchair for the chest radiography. The wheelchair was "backed up" to the DR vertical image receptor and the patient's chest was imaged in the AP position. This was considered to be easier and safer than the alternate chest imaging techniques. There is an artifact across the top of the patient's chest from the edge of the wheelchair material. (cardiomegaly, sternal sutures, atelectasis, consolidation, pleural effusions and cardiac prosthetic valves noted)


6. AP Sitting Chest Radiography- Position of Scapulae
7. AP Sitting Chest Radiography- How Upright?
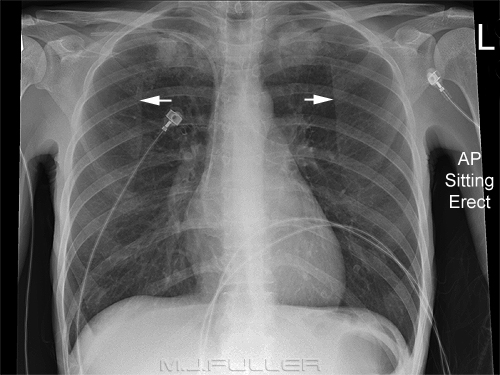
This patient has undergone bedside chest radiography in the AP sitting position. The scapulae are superimposed over the lungfields. It is well recognised that the scapulae can be "rolled forward" in the PA erect position. It is less common to see radiographers attempt to achieve the same result in the AP sitting position. This patient also has been positioned in the AP sitting bedside position. The radiographer has asked the patient to reach forwards and internally rotate her hands. This has resulted in good clearance of the scapulae from the lungfields.


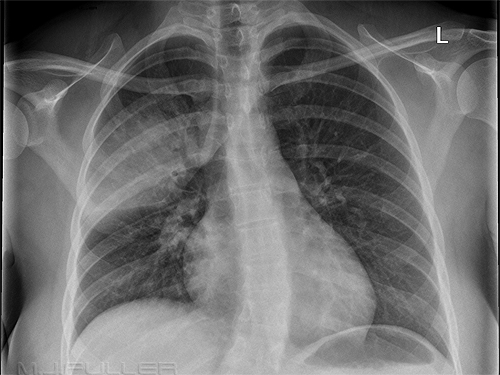
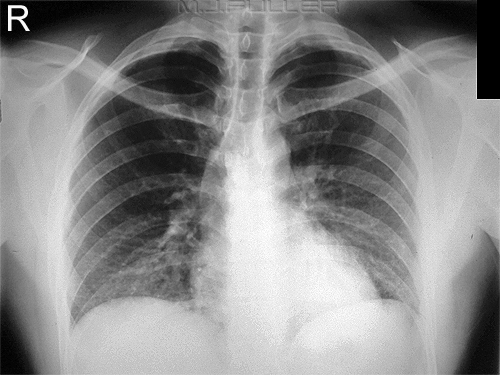
This patient presented with exacerbation of COAD to the ED. There is evidence of COAD, bullae and atelectasis. The patient has undergone bedside chest radiography in the AP sitting position. The question often arises as to the benefits of achieving a fully erect AP sitting position- why not just angle the X-ray tube to suit the semi-erect position of the patient?
In this case, the use of an angled beam has failed to demonstrate the air/fluid level in the infected bullae.A lateral view image demonstrates several fluid levels. The fluid levels are relatively easy to detect on the lateral view because a horizontal X-ray beam was employed. The fluid levels are difficult to detect on the AP sitting image because of the caudal tube angle employed.
This is not an argument for employing a horizontal tube for all bedside chest radiography. Rather, the case suggests that a horizontal ray technique could be important in cases where air-fluid levels may exist and also identifies the potential value of the lateral view.
Burgener et al suggest benefit in demonstrating an air/fluid level on both AP/PA and lateral views



8. Assess Your Entire Image
9. Beware Artifacts
When assessing your image it is worth considering the radiology as well as the radiography. There are sometimes findings that need to be relayed back to the referring doctor for urgent attention (e.g. pneumothorax, flail chest, tension pneumothorax). In this case, the patient has an unexpected dislocated shoulder that had been missed on earlier chest imaging.

10. Markers and Text
The faint arrowed structure could be mistaken for a bone lesion or a solitary pulmonary nodule. It is in fact neither- it is a plastic ECG dot.... beware This patient appears to have unusually dense breast shadows. This is a legacy of breast augmentation. The margin of the left breast implant is arrowed.


11. Side Markers
If you are using digital markers or post-processing text why place it over the patient's anatomy? There is always a chance that you will obscure an important lesion
(breast augmentation noted)The radiographer has positioned the post-processing digital text very close to the pathological fracture (my arrow) of the left clavicle.... why not position the text so that it does not overlay the patient's anatomy?
The placement of the digital text over the left humeral head is undesirable and unnecessary.
-colonic interposition or Chilaiditi Sign (Pronounced “Ky-La-Ditty”) notedThe placement of the side marker has resulted in it encroaching on the left head of humerus. This is sometimes difficult to avoid on a PA/AP chest x-ray. By contrast, the placement of the digital text over the left humerus is easily avoidable. In this case, the digital post-processing text is overlying the left humerus which is showing signs of tumour secondary deposits. There is space for this text to be positioned such that it does not overly bony anatomy.



12. Paediatric Chest Radiography
A patient arrived in the resus room following a transfer from a regional hospital. The patient arrived with this image.
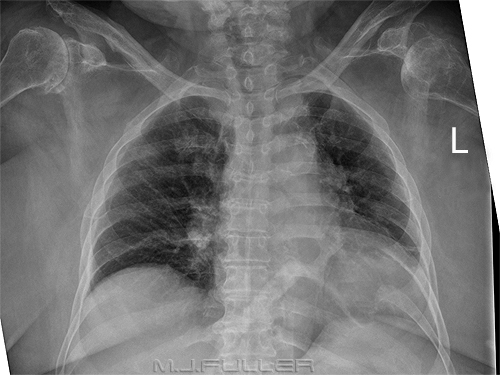
Question: What is missing?
Answer: Patient name and side markerIt was decided to repeat the chest radiography. The image shown above demonstrates that the patient has dextracardia. This finding was not appreciated on the original film because of a lack of side marker. Beware.


13. Arm Abduction
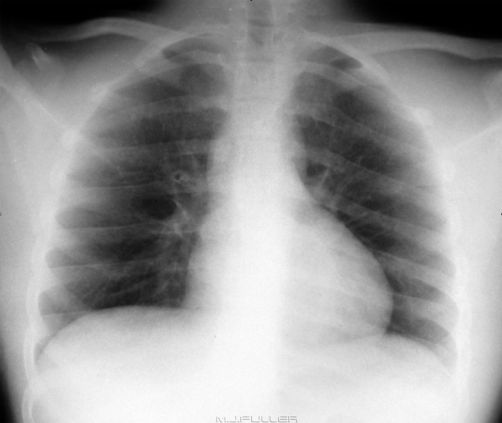
This is a lateral chest X-ray image of a child. Note that the child's back is vertical. If the patient is imaged for the AP projection in the same position with a horizontal beam, up to one third of the child's lungs will be hidden behind the hemidiaphragm. This is the actual position in which the child was imaged for both the AP and lateral projections. A 15 degree sponge has been placed behind the child's back to effectively lean the patient forward.


14. Beam Collimation
This is an AP sitting chest image. The patient's left arm is not abducted sufficiently resulting in overlap of the soft tissues of the arm over chest anatomy. A minimum of abduction of the patient's arm will overcome this problem.
The Serratus anterior muscle can also produce an opacity that may resemble pleural tickening. This is sometimes referred to as a "bowling-pin" silhouette.
"When the muscle is well developed, the medial edge of this silhouette may be superimposed upon the air shadow of the lung in a variety of ways. When it overlies the apex of the lung, it gives rise to the companion shadow; when overlying the midlateral lung edge and costophrenic angle it may mimic pleural and/or extrapleural disease. Recognition of the various possible patterns is important to prevent overdiagnosis of disease, particularly asbestosis."
<a class="external" href="http://www.ncbi.nlm.nih.gov/pubmed/441365" rel="nofollow" target="_blank">
</a><a class="external" href="http://www.ncbi.nlm.nih.gov/pubmed/441365" rel="nofollow" target="_blank">Gilmartin D.The serratus anterior muscle on chest radiographs. Radiology. 1979 Jun;131(3):629-35.</a>
-colonic interposition or Chilaiditi Sign (Pronounced “Ky-La-Ditty”) notedThis patient has her hand overlying the left lower lobe. It is good practice when undertaking bedside chest radiography to with-hold exposure until you can see both of the patient's hands.

This is an AP sitting chest image. 4-way collimation is rarely seen in chest radiography. One method that radiographers' employ to good effect is to collimate no wider (laterally) than the AC joints. Note that the lateral collimators are opened exactly to the AC joints.
Tight collimation reduces patient dose and scatter radiation. The improvement in image quality is most noticeable in morbidly obese patients.

15. Aluminium Filters in Chest Radiography
This is a PA erect chest radiograph on a lady with large breasts. The costophrenic angles are just visible but underpenetrated. This is the same projection of the same patient using an aluminium filter. The differences may appear subtle at first. Compare the costophrenic angles and the heart shadow. You would have a much better chance of diagnosing a left lower lobe pathology on this image than the one without the aluminium filter.
Note that this is a radiograph rather than a digital image. The benefits of utilising an aluminium filter are considerably less when a digital technique is employed (CR or DR).


16. Single View Chest Radiography
This is a PA/AP chest image on a paediatric patient. It may be tempting in a difficult patient to finish the examination at this point. The lung fields are well demonstrated and you can even see behind the heart and under both hemi-diaphragms. This is a lateral chest image on the same patient. Note the left lower lobe consolidation. In retrospect, there is increased opacity seen behind the heart on the AP view, but this could easily be missed.
Any single view radiography is hazardous, and the chest is no exception.
There is further discussion on the value of a lateral chest image here.


17a. The Value of Good Inspiration - PA
This patient has increased opacity in both lung bases. The difficulty with this image is that it is difficult to know how much of the basal opacity is due to crowding of lung structures and how much is pathological.
The problem can be technique related. There can be a tendency for radiographers to ask the patient to "breathe in and hold your breath" without actually watching the patient to see when they have completed their inspiratory effort. Don't "kick in the autopilot" when giving the patient breathing instructions- watch what the patient is doing.This is the same patient who has been encouraged to take a deeper breath in. The basal lung structures have been separated enough to be confident that there is no basal pathology.


17b. The Value of Good Inspiration - Lateral
This lateral chest image demonstrates very poor inspiration. The diagnostic value of the image is reduced significantly.
(extensive artifact and rotation noted)This is the same patient who has been encouraged to take a deeper breath in. All of the lungfields and mediastinum are showing improved demonstration.


18. The Value of Viewing old Chest Radiography Before you Start
Patients who have unusual chest anatomy tend to have radiographic errors repeated when the radiographers don't check old imaging before they start.
It is common practice in Australia for Radiographers to tell patients when they have "long lungs". There have been many occasions when a patient has said to me "... the last time I had a CXR the radiographer advised me to tell you that I have long lungs". This is a simple effective practice.Whilst some patients have long lungs, others have wide lungs. Despite a valiant effort by the radiographer to fit the chest anatomy with the cassette in portrait orientation, landscape cassette orientation would have been a better choice.

19. The Value of Comparison with Old Chest Radiography
This 18 year old male presented to the Emergency Department with headache, fever and viral signs. There is increased opacity of the left lung behind the heart shadow. This is easier to appreciate when compared with the normal CXR taken 2 years earlier (right). This is the type of subtle pneumonia that is easily missed- when the patient represents 3 days later they are considerably sicker! This CXR from two years earlier demonstrates a normal LLL. The lateral projection image similarly demonstrates a very subtle sign of consolidation. The thoracic vertebral bodies should show an evenly graduated darkening from the top to bottom. This image demonstrates a few slightly lless dense thoracic vertebral bodies behind the heart. Compare with the lateral chest image taken a few years earlier. Normal lateral chest X-ray taken a few years earlier.




20. Radiography of 'Big Lungfields'
Patients who have very large lungfields can present a challange to the radiographer. There are a number of radiographic considerations which should be remembered 1. If you routinely check old imaging you will be aware that the patient has large lungfields before you start
2. COPD patients have physical characteristics (barrel chest, SOB ec) that should lead you to expect large lungfields
3. If you have access to DR imaging that can achieve a 43 x 43 cm (17 x 17 inches) this should be utilised
4. COPD patients will require considerably less radiation exposure
5. Let the patient know they have large lungfields and ask the patient to let the radiographer know each time he/she has chest radiography.The cassette may need to be positioned landscape for lateral chest radiography.

21. Bedside Chest Radiography of Non-compliant Patients
There is a level of compliance that is required for most radiographic examinations and bedside chest radiography is no exception. There is a case for advising the referring doctor that satisfactory and safe chest radiography will not be possible with the patient's current level of non-compliance. This will ensure that the referring doctor will either increase the patient's level of sedation or reconsider the need for the X-ray examination where increased sedation is not tenable.
Producing an image such as this one is a largely pointless exercise- where there is a low likelihood of success, it is prudent to consider alternative approaches including abandoning the examination.

22. Non-compliant Patient with a Necklace
This patient presented to the Emergency Department with a suspected chest infection and was referred for chest radiography. The radiographer noted that the patient was wearing a heavy metal chain around his neck. The patient refused to remove the chain, but was willing to support the chain off his chest by holding it in his mouth. This technique can be used with any patient for chest radiography who is unwilling and/or unable to remove the chain/necklace. The presence of the chain around the patient's neck is less of a problem in the lateral position


Summary
Plain film radiography is not considered a particularly 'sexy' imaging modality today and chest radiography even less so. Despite this, plain film radiography remains the mainstay modality of many imaging departments and chest radiography is usually the most common plain film examination. Not unlike any other area of medical imaging, it can be done well or badly, and deserves the attention and effort of radiographers to achieve the best possible result.
References
....back to the Applied Radiography home page
1. T M BERNHARDT, MD, U RAPP-BERNHARDT,U W KRAUSE, MD and W DOEHRING, MD. Digital selenium radiography:radiography in a clinical study. The British Journal of Radiology, 73 (2000), 963±968 E 2000 The British Institute of Radiology
<a class="external" href="http://bjr.birjournals.org/cgi/reprint/73/873/963" rel="nofollow" target="_blank">http://bjr.birjournals.org/cgi/reprint/73/873/963</a>2. HIROSHI SATO, TAKAHITO KATANO, YOSHIFUMI NAKAMURA, and YOSHIAKI KITAMURA. Study of Chest Portable Radiography using Computed Radiography: Removal Effect of X-ray Scatter by a Copper Plate. Jpn J Radiol Technol 2001; 57 (4) : 433-439 3. ROBERT G. GOULD M.S. and JOHN HALE PH.D. CONTROL OF SCATTERED RADIATION BY AIR GAP TECHNIQUES: APPLICATIONS TO CHEST RADIOGRAPHY, American Journal of Roentgenology