Neck of Femur Fractures
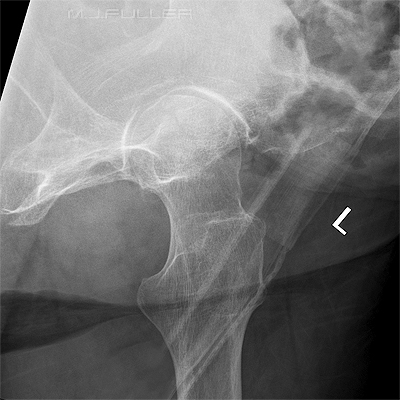
AP Hip- Leg Externally Rotated
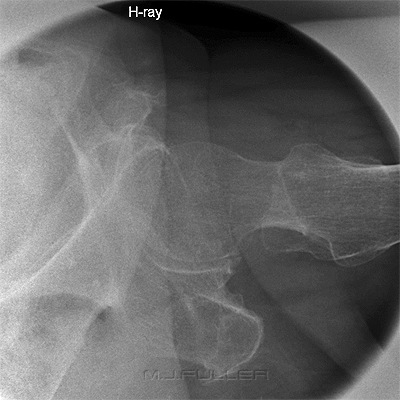
True AP Hip Position Leg Internally Over-rotated
With the patient's legs externally rotated, the greater trochanter
is partially superimposed over the femoral neckWith the patient's legs internally rotated, there is maximum visualisation of the femoral neck
Internal rotation of the patient's leg can be over-done.
This patient's legs have been internally rotated to a degree that
the patient's lesser trochanter is not demonstrated
Comment.It is commonly necessary for the radiographer to start a trauma hip X-ray examination on the assumption that the patient has a neck of femur fracture or other hip/pelvis fracture. It is therefore not initially appropriate for the radiographer to internally rotate the patient's affected leg for the AP hip/AP pelvis view. If the AP hip/AP pelvis image does not clearly demonstrate a fracture, and there is no evidence of other fracture of the affected leg, it may be appropriate to internally rotate the effected leg with the patient's consent and perform a repeat. Radiographers are sometimes criticised for not internally rotating a ?NOF patent's affected leg, when in fact it was appropriate not to do so for the initial imaging.






Shenton's Line
Shenton's line is a line formed by the inferior aspect of the superior pubic ramus and the medial aspect of the upper femur. Shenton's line should describe a smooth curve. If there is any sharp angulation of Shenton's line the patient could have a neck of femur fracture. An abnormal Shenton's line can be the most obvious indicator of a patient's fractured neck of femur demonstrated on an AP pelvis /hip image.

Modified Rolled Lateral Hip I (Unilateral Cleaves or Frogleg Position)
Raised Knee Lateral Hip Image
Raised Knee Lateral Hip Positioning
This technique demonstrates the neck of femur clearly. One of the advantages of this position is that it utilizes the table bucky/IR and benefits from the associated image quality.
Note mattress artifact.This position is similar to that employed with a rolled non-trauma lateral hip. The only difference is that the patient's knee on the affected side is raised off the table and rested on a positioning sponge. The suggested angle between the femur and the tabletop is approximately 30-35 degrees. If you increase this angle (up to 45 degrees), you will achieve even greater clearance of the trochanter off the femoral neck, however, you will also increase the elongation/distortion of the femoral neck


Raised Knee Lateral Hip
This technique demonstrates the neck of femur clearly. Compare this technique with the conventional rolled lateral hip image (right)
This is a conventional rolled lateral hip image. The greater trochanter almost completely obscures the femoral neck rendering it an unsuitable view for trauma radiography of the hip.
Raised Knee Lateral Hip Image
Conventional Lateral Horizontal Ray Trauma Hip
This technique compares favourably with a conventional lateral
horizontal ray trauma hip technique (see image on right)This is a conventional horizontal ray trauma hip image. The demonstration of the femoral neck compares favourably in this image with the "raised knee" lateral (left). Merrill's refers to this as the "Danelius-Miller method".




Modified Rolled Lateral Hip II (Friedman Method)
Modified Lateral Hip Image
Modified Lateral Hip Positioning
This technique is very similar to the previously described modified lateral hip technique. The difference is that the tube is angled instead of the anatomy (the effect is virtually identical).
The patient position is identical to a conventional rolled lateral hip. The only difference is the use of a 30-35 degree cephalic tube angle. Of course, unless you give the full 45 degrees of cephalic angle, there will be some superimposition of the greater trochanter over the neck of femur. Experience suggests that a 45 degree cephalic angle produces too much distortion of the femoral neck.



Modified Rolled Lateral Hip II (Friedman Method) at Various Tube Angulations
These images demonstrate the effect of increasing the cephalic angulation on the femoral neck. As the cephalic angle is increased the greater trochanter is increasingly projected off the femoral neck. Experience has suggested that a maximum of 35 degrees cephalic angulation provides the best compromise between projecting the greater trochanter off the femoral neck and distortion/elongation of the femoral neck.

Modified Rolled Lateral Hip III (Modified Friedman Method)
Raised Knee and Cephalic Tube Angle Lateral Hip Image
Raised Knee and Cephalic Tube Angle Lateral Hip Technique
This position is a combination of the two previous modified lateral hip techniques. The patient is positioned as shown above with a slightly raised knee (15-20 degrees) and a smaller cephalic tube angle (15-20 degrees).


Horizontal Ray Lateral hip
Technique 1
This is a commonly employed lateral horizontal ray hip radiography technique. This technique is ideal for patients who present to the Emergency Department with suspected neck of femur fracture. A stationary grid is usually employed with grid lines orientated horizontally. The contralateral (unaffected) hip is flexed and abducted with knee flexion. The unaffected leg can be supported /rested on a suitable support. This is a lateral horizontal ray hip image. The radiographer has used a round cone.
Vascular calcification noted.


Technique 2
This technique is similar to technique 1 except that the patient is angled rather than the central ray. This tends to result in a large 'air gap' with associated increase in X-ray exposure. These considerations should be balanced with the improvement in quality associated with a wall bucky/ DR IR. Thereduced scatter associated with an airgap will allow a non-grid technique to be employed in some patients. This is a horizontal ray lateral hip image using the central ray at right angles to the IR. The DR wall receptor was employed rather than a cassette and stationary grid. The patient was positioned as described above left.


Clinical Presentation
Clinical appearances such as this should be considered indicative of a fracture, not diagnostic of a fracture. This false appearance of NOF fracture is a result of external rotation and slight knee flexion.Patients with neck of femur fractures commonly present with Patients are commonly referred for ?NOF fracture hip radiography despite the fact that the patient does not have a neck of femur re previous hip replacement surgery. These are commonly patients who have not been examined by the referring doctor. Radiographers should provide encouragement to the referring doctors to examine their patients prior to referring them for radiography. A sound clinical examination (when possible) will help to ensure appropriate and economical radiography.
- a history of falling over
- one leg shortened and externally rotated
- patients are usually elderly

Case 1
This 93 year old male presented to the Emergency Department after falling at the nursing home. His right leg was shortened and externally rotated. He was examined and referred for right hip radiography.
Shenton's line demonstrates abnormal contour on the right suggesting a neck of femur fracture. (see below)Shenton's line should be a smooth curve- the angulation in Shenton's line suggests a neck of femur fracture. There is also a discontinuity in the lateral aspect of the right neck of femur (arrowed). The radiographer performed a 25 dergree (sic) cephalic angle projection of the right hip. This projection clearly demonstrated the neck of femur fracture (arrowed). This is a very useful projection in cases of equivocal fractured neck of femur.
Normal lateral hip for comparisonThe horizontal ray lateral projection was performed with a stationary grid. There is a cortical discontinuity of the superior aspect of the neck of femur (arrowed). Compare with the normal lateral neck of femur image below .




... back to the Wikiradiography home page
... back to the Applied Radiography home page