Lateral Soft Tissue Neck for Foreign Body
Case StudiesIntroduction
Soft tissue neck radiography is less of a positioning challenge than an interpretation challenge (in a cooperative patient). This page is dedicated to the radiography and image interpretation challenges of soft tissue neck radiography.
Radiographic Technique (lateral)
The radiographic positioning is similar to a lateral cervical spine. The patient can be imaged in the erect or supine position as dictated by the patient's condition. As much relevant clothing and jewelery should be removed. Typically, shirt collars and earrings produce artifacts. Even a t-shirt collar can produce an artifact. The patient should be in the true lateral position and the patients neck should be comfortably extended (except in cases of neck trauma). The patients shoulders should be as low as possible.
Exposure should be made at the end of inspiration to ensure that
- The pharynx/airway is fully outlined with air
- The soft tissues are not distorted
- the patient is not swallowing during the exposure
The arrowed soft tissue structure is a legacy of exposing on expiration. Irrespective of the reason for performing a lateral soft tissue neck view on this child, this appearance is not helpful in terms of the diagnostic quality of the image.
If a paediatric patient is imaged at full expiration, the retropharyngeal soft tissues can appear to be falsely widened. Equally, if the patient is swallowing during the exposure, the upper phayngeal airway can appear narrowed.
If you are using non-digital equipment, the exposure should be for soft tissues rather than bone. This is to say, this is not a lateral cervical spine exposure.
In cases of severe retropharyngeal abscess, the abscess can extend into the patient's mediastinum. It is prudent to perform PA and lateral chest radiography in these patients.

Case 1

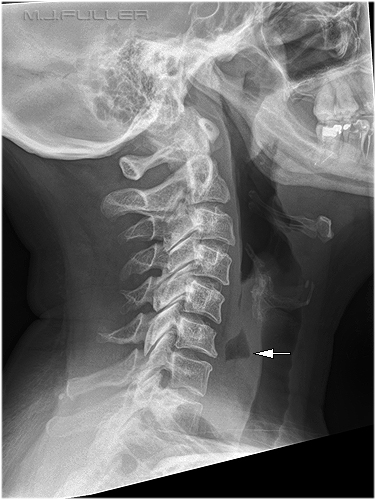
This patient was eating a seafood dish and swallowed something hard. It was suspected to be a piece of mollusk shell. The lateral soft tissue neck revealed a piece of shell in the pharynx at the origin of the oesophagus (arrowed)
Stylohyoid ligament calcification noted.
Case 2
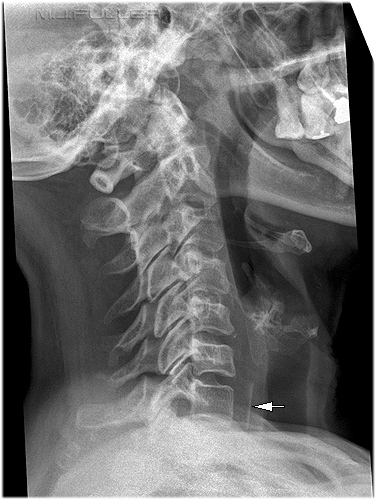
This patient presented after eating meat and was complaining that a piece of meat was stuck in her throat. There is a faint irregular mottled density in the oesophagus with an air-fluid level seen immediately superiorly to this density (arrowed). The mottled density was assumed to be the meat causing the air-fluid level. Air in the oesophagus can be a normal finding associated with air swallowing. The air-fluid level in this case was suggestive of an obstruction in the oesophagus.
Case 3
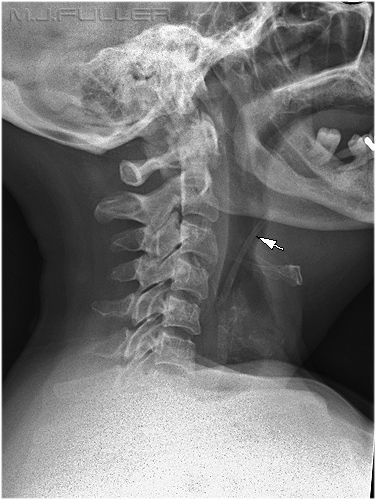
This patient presented with a sensation of something stuck in her throat after eating a chicken and salad meal. There is a linear density if the oesophagus consistent with a piece of chicken bone (arrowed)
Note that the patient's head and neck are not in the true lateral position.
Case 4

This child presented after swallowing a coin. The coin is lodged in the upper oesophagus.
Case 5
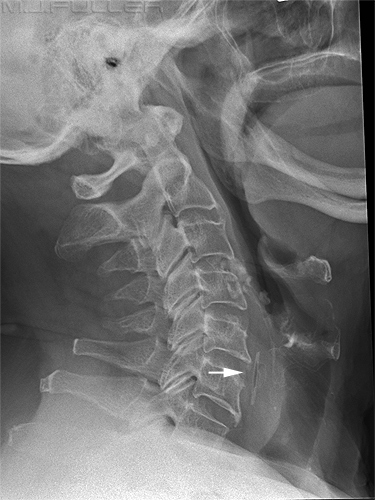
This patient presented after eating chicken. She reported a severe and painful sensation of something stuck in her throat. The arrowed structure is a chicken bone in her pharynx.
Case 6
The arrowed structure is a tablet which is still in its foil packaging. This foreign body is stuck in the patient's oespophagus. There appears to be some soft tissue swelling associated with the foreign body.
Case 7
The arrowed structure is food in a Zenker diverticulum. Bra hardware and clothing artifact noted.
The nature of a Zenker Diverticulum is detailed below
"Problem: The esophageal mucosa herniates posteriorly between the cricopharyngeus muscle and the inferior pharyngeal constrictor muscles; therefore, Zenker is a false diverticulum. This diverticulum carries with it a high frequency of food elements retained within its pouch. These food elements and secretions lead to halitosis, regurgitation, aspiration, and dysphagia.
Etiology: It is thought that patients with Zenker diverticulum have improperly timed relaxation of the cricopharyngeus muscle during swallowing. Over time, the increased pressure causes herniation of the esophageal mucosa posteriorly, between the inferior pharyngeal constrictor and the cricopharyngeus muscle. Whether these patients have an anatomical predisposition to diverticulum formation is unknown.
Pathophysiology: Abnormal muscle activity in the cricopharyngeus results in a discoordination of the swallowing mechanism that causes increased pressure on the mucosa of the pharynx. This results in the slow, progressive distention of the mucosa. The weakest area is posterior, the location of the pulsion diverticulum formation."
<a class="external" href="http://www.emedicine.com/med/topic2777.htm" rel="nofollow" target="_blank">http://www.emedicine.com/med/topic2777.htm</a>
Case 8

This patient has extensive subcutaneous emphysema (abnormal air in the soft tissues of the neck). The causes are various but would include surgery, trauma, pneumothorax, infection and pneumediastinum.
Case 9
This 60 year old male presented to the Emergency Department with a sensation of a foreign body stuck in his throat following a meal. The patient was examined and soft tissue neck radiography was requested.
There is evidence of a metallic foreign body in the upper oesophagus. The appearances suggest the foreign body may be wire.
The routine projection for soft tissue neck at this institution was lateral only. The radiographer considered that the localisation of this foreign body required an AP projection. This was likely to be successful given the metallic nature of the foreign body.This is a magnified presentation (photographic magnification) of the foreign body. The wire appears to be tied in a knot. The AP projection confirms that the possible foreign body is midline and is therefore likely to represent an ingested metallic foreign body in the upper oesophagus. Note that the appearance of a knot in the wire was projectional only.












The black arrow is pointing to stylo-hyoid ligament calcification x2. This is very common and variable in its appearance.
The grey arrow is the hyoid bone

There are hair clips, ear rings, and a bra clip noted. It would not be difficult to imagine that larger earrings would have obscured anatomy of interest.
The arrowed structure is a shirt collar. The shirt is best removed for the lateral soft tissue neck projection

Summary
....back to the applied radiography home page hereThe lateral soft tissue neck is similar in its positioning to a lateral cervical spine. It is helpful to remove all artifact-producing clothing and jewelery from the patient. Exposure should be made at the end of inspiration. It is important to establish what are the normal anatomical features ( hyoid bone, cricoid cartilage, thyroid cartilage, stylo-hyoid ligament calcification, pseudo soft-tissue swelling) and what are abnormal features (foreign body, pathological soft tissue swelling)