Imaging Nail Gun Injuries
Nail guns are devices that take the hard work out of jobs that require large amounts of nailing. When building a timber framed house, literally thousands of nails are used to join the timbers. You can hazard a guess as to the risks that a carpenter would face in a 12 month period of using a nail gun (multiply that by 40 years for a working lifetime)
The Nail Gun
| | There are large numbers of nail gun types used in the building industry. This graphic demonstrates the safety mechanism typical of most pneumatic nail guns (known as "bump" guns in the industry). The important safety principle that is featured with this type of nail gun (and many other power tools such as hand-held circular saws) is that you must make two actions simultaneously for the nail to exit the gun. The rationale is that you might accidentally activate one of the triggers, but you are less likely to accidentally activate both triggers at the same time. I have it on good advice from my colleague (carpenter turned radiographer) that when you are using a clout gun to nail roof rafter straps, it is very convenient to keep your finger on the trigger and just use the catch release trigger (the bump) to activate the piston that pushes the nail into the timber. In terms of safety, you are now down to one trigger. If you are not concentrating, you can put the nail gun down while you still have your finger on the trigger. If you happen to touch the catch release trigger on your leg (bump) on the way down..bingo- nail in the femur. Equally, if you fall or lose your balance and you have your finger on the trigger, instant stigmata. An alternative to keeping your finger on the trigger is to bypass the bump mechanism such that when you pull the trigger the nail is fired- a reliable method of losing your builders licence if you are caught! |
|

Google's Offering
A quick search of google reveals a smorgasbord of nail gun injuries
<a class="external" href="http://img2.timeinc.net/toh/i/g/0807_nailgun/nail-gun-hand.jpg" rel="nofollow" target="_blank">http://img2.timeinc.net/toh/i/g/0807_nailgun/nail-gun-hand.jpg</a>
<a class="external" href="http://img2.timeinc.net/toh/i/g/0807_nailgun/nail-gun-foot.jpg" rel="nofollow" target="_blank">http://img2.timeinc.net/toh/i/g/0807_nailgun/nail-gun-foot.jpg</a>
<a class="external" href="http://www.taproot.com/blog/Nail+Gun+Knee.jpg" rel="nofollow" target="_blank">http://www.taproot.com/blog/Nail%20Gun%20Knee.jpg</a>



What the Surgeon Wants to Know.
The nail is usually surgically removed from the patient. If the nail head is visible, localisation is not a problem. If the nail head is not visible, an entry point skin marker is required. The radiographer's job is to identify the position of the nail and, importantly, determine if it is embedded in bone. If it is in bone, it will have implications for
- surgical removal
- washout of the wound
- antibiotic therapy
- follow-up recommendations
- associated fractures
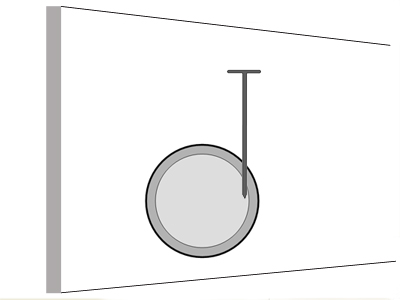
This is not the actual patient from this case study, but the similarities are remarkable.... the only difference I could see, was that my patient wasn't doing much waving.
Note that the nail is insitu in the patient's right leg supero-laterally to the patella. The patient's clothing has been cut with a patch left around the nail head.

This was the first image produced. This is a lateral horizontal ray knee projection. There were technique limitations associated with the patient's fixed knee flexion. Unfortunately, this image does not answer the most important question - is the nail embedded in the patient's femur?
What is arguably required is one projection that is perfectly en face and one that is perfectly tangential.

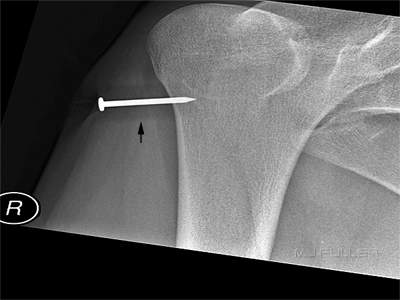
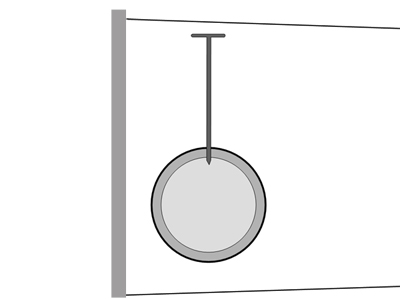
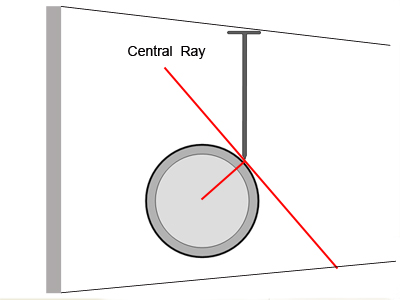
This image was an attempt to produce a projection that captured the nail tangential to the femur (in perfect profile). The black arrow is pointing to an artifact (? blooming artifact). The visible head of the nail provided the radiographer with a guide as to how to direct the X-ray beam such that it was orientated tangentially as shown in the graphic. The nail appears to have entered the bone. It is useful if the patient has a nail with them to use as a guide. You can gauge how well you have the nail in profile if you know how thick the head is. Not all nails will have a head large enough to gauge thickness.
This is the projection that you are aiming for.


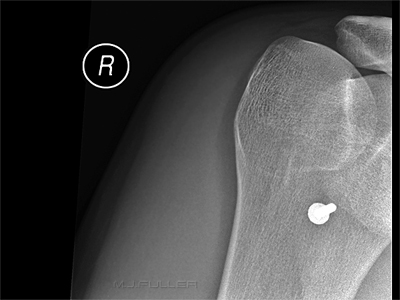
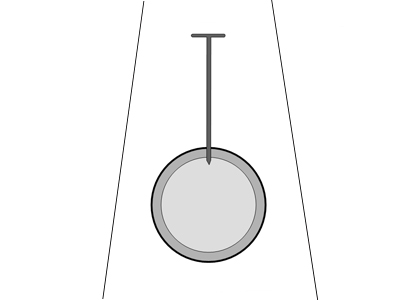
If you achieve a perfect en face position (with respect to the head of the nail), the head of the nail will be concentric with the shaft of the nail. This projection is not perfect, but very acceptable in practical terms. This projection is required to be considered in conjunction with the tangential projection. Without this projection , the tangential projection is meaningless (see below for explanation).
This is the position that you are aiming to achieve.
The surgeon was not initially satisfied with these views. The positioning was not conventional. When I explained why these projections were chosen, he decided that he did not want any more imaging (good communication is often the answer). I discussed the case with him and suggested that the image intensifier (during surgery) may provide additional confidence that the nail was embedded in the patient's femur. I saw the surgeon the next day and he confirmed that at surgery he found that the nail was embedded in the distal femur- game over. He did not require the image intensifier during surgery because he could "...see that the nail was in the bone".
Why do you Need the en face Projection?


Image 1
Image 2The reason that you need the en face view is that you can't be sure whether a nail that appears to be in bone on the tangential view is in fact sited in the bone or alongside the bone. This is the basic principle of foreign body localisation- you need two views at ninety degrees (right angles). Furthermore, you are also interested in any associated fractures which could easily be hidden on a single image.
This image will appear very similar in a tangential projection to the same projection of the embedded nail (see image 1)


Case 2

This is not a dissimilar injury to that seen in Case 1. The radiographer has performed two initial conventional knee projections- AP and lateral. It is unclear whether the nail is embedded in the femur in this view alone.


The AP projection of the knee demonstrates that the nail has deflected off the cortex of the femur. Importantly, the tip of the nail (the pointy end) is clear of the femur. There is no projection that will project the tip of the nail clear of the femur if it is actually within the cortex or medullary cavity of the femur.
Note that the nail head is not a complete circle in shape- it is "D" shaped.
The radiographer considered that the relationship between the nail and the cortex of the femur could be demonstrated better.




Angles were measured using the CR software with a view to projecting the nail completely clear of the bone using compound tube angles. I'm not convinced that this exercise added any new information, but it was an interesting exercise nevertheless.
Other Nail Orientations
It is possible that the nail may not be pointing directly at the centre of the long bone as show below. How will this affect imaging?
An en face/axial projection of the nail and a projection at right angles to the enface/axialprojection will show the nail as embedded in the femur. A true tangential projection such as that shown below will probably require the assistance of an image intensifier.
This nail position is less likely to occur because of the tendency for the nail to deflect off the cortex.

This nail position presents more of a challenge in terms of demonstrating its true position in relation to the femur. The true tangential view demonstrated in this graphic will be best achieved with the aid of an image intensifier.
If the head of the nail is visible, you should be able to make a assessment of the nail's general orientation.
It might also be clear that the nail is not in the bone because of its ease of extraction.

Case 3
This patient presented to the Emergency Department with a nail from a nail gun in his foot. He had lost his balance while building a house frame. He fell over with the nail gun in his hand and his finger on the trigger. The rest is self-explanatory.
Taking into consideration:
- the known length of the nail
- the amount of nail that is protruding
- the angulation of the nail
- the entry site
... the nail is in the second metatarsal until proven otherwise
The light coloured irregular material attached to the nail is a glue that keeps the nails together in rows prior to firing. Some nails have a glue that is designed to melt on entry into the timber from the associated heat from friction. On cooling, the nail is effectively glued into place.


positioned for lateral cross-table view
Lateral cross-table foot view. Position is modified slightly to centre on the nail. Centring on the nail reduces parallax error


The AP (DP) foot image does not conclusively confirm that the nail is embedded in the head of the second metatarsal
The appearance of a fine black line "halo" around the nail is artefactual- an edge enhancement artifact caused when the image was prepared for posting on the WWW in Photoshop. This is referred to as halation or uberschwinger artifact. This artifact can be mistaken for evidence of loosening of an orthopaedic device (note this nail isn't loose- was just shot in an hour earlier).
Further Reading- <a class="external" href="http://bjr.birjournals.org/cgi/reprint/70/832/431" rel="nofollow" target="_blank">http://bjr.birjournals.org/cgi/reprint/70/832/431</a>
This is not a Mach Band - when you enlarge the image in photoshop you can see the black line.
When the AP projection image is examined at full resolution, there is evidence of "breakout" of the cortical bone as the nail has exited from the second metatarsal (subtle)
Note that the black "halo" line around the nail is not visible on this full resolution view
When this reverse oblique view is considered with the lateral view, it is highly convincing that the nail is embedded within the head of the second metatarsal



Case 4
Source: Haakon Hjemly, Wikiradiography images
Reproduced with permission
The history associated with these images is unknown. It would be a fair guess that the operator inadvertently fired a nail into his/her foot through a steel-capped boot. As is often the case, the nail head is located flush with the patient's skin. Plain film X-ray imaging would appear to be a prudent precaution prior to removal of the patient's boot.
Source: Haakon Hjemly, Wikiradiography images
Reproduced with permissionFurther imaging post boot removal would be required to determine if the nail is located within bone/joint. Alternatively, an image intensifier assisted removal would provide the same information.


Case 5
This patient presented to the Emergency Department after falling with a nail gun in his hand.
The AP knee projection was taken with the patient's knee in slight flexion. The position of the patella suggests the knee is slightly internally rotated.
These two projections at 90 degrees suggest that the nail is embedded in the patient's distal femur. The radiographer attempted to provide further evidence by producing an image with the central beam along the axis of the nail as shown below.
The attempted 'axial nail' view was only partially successful given that the entire nail was not included in the image. Despite this limitation, this projection did support the contention that the nail was embedded in the distal femur.



Case 6
This patient presented to the Emergency Department with a nail from a nailgun in his thumb. The nail was accidentally fired into his thumb at a building site. The nail appeared on visual inspection to have missed the terminal tuft. Radiography of the thumb was requested to confirm the position of the nail in relation to the adjacent bony anatomy.
Standard PA and lateral projections were performed. In addition, an axial nail position was attempted. It was clear that a true axial nail position would cause the head of the nail to be superimposed over the area of interest. A compromise off-axial position was utilised. It appeared at this stage that the nail had passed through the distal phalanx. The radiographer was not satisfied given the clinical appearance of the nail missing the bone.
Further imaging was warrantedA final attempt to demonstrate the nail clear of the bone was attempted. This position is not a conventional radiographic position. The patient's thumb was positioned in a hitch-hikers position (abducted) and was pointing straight down towards the IR. An off-vertical central ray was utilised to produce a semi-axial projection.
The image demonstrates the nail to be located in the soft tissues of the thumb.
On review, it would have been useful to remove the head of the nail with bolt cutters and produce a true axial projection of the nail.


Case 7
This patient presented to the Emergency Department with a nail from a nailgun in his left hand. The nail had deeply penetrated his left hand and could conceivably be embedded in bone. He was referred for radiography of his left hand. The PA projection image demonstrates the tip of the nail superimposed over the base of thumb and trapezium. The oblique hand projection image demonstrates the tip of the nail projected over the base of the second metacarpal. These 2 images alone suggest that the nail is not embedded in bone. The lateral hand projection image is inconclusive. The routine projections of the patient's left hand provided compelling evidence that the nail was located within soft tissue only. The radiographer considered that a semi-axial projection of the nail may show the entire length of the nail clear of bone- this was achieved. The patient's hand position was PA with wrist flexed.






Case 8
This patient presented to the Emergency Department with a nail from a nailgun in his right hand. The nail had passed through the second and third digits of his right hand.
The nail could be embedded in bone. He was referred for radiography of his right hand.
The AP oblique projection image suggests that the nail could be within the bone of the middle phalanges of the second and third digits.
There is blooming artifact surrounding the nail and side markerSimilarly, the lateral hand projection image suggests that the nail could have passed through the middle phalanges of the second and third digits. The radiographer has attempted to position the patient's hand such that an axial demonstration of the nail was achieved. In doing so, the radiographer realised that the head of the nail would, in all likelihood, overly the bony anatomy that needed to be demonstrated. A compromise position was achieved to project the head of the nail off the palmar aspect of the second middle phalanx.
This position has successfully demonstrated that the nail has passes through the soft tissues of the second digit (probably avoiding flexor tendons).The radiographer has not proven whether the nail has passed through the middle phalanx of the third digit. An axial nail type position was attempted with the head of the nail projected in the opposite direction to that shown above.
Considering the first PA oblique hand image, it was known that only the tip of the nail could have come to rest in the middle phalanx of the third digit. This projection demonstrates that the tip of the nail is not embedded in bone.
CommentThe nail could have been demonstrated clear of bone by removing the head of the nail. It was decided not to pursue that avenue given that there was compelling evidence that the nail had not passed through bone. In addition, there was no evidence of associated bony injury/fracture which you might expect of the nail had passed though bone.
The radiographer should label the digits on the images for ease of identification.




Case 9
This 31 year old male presented to the Emergency Department following a nailgun injury. On examination, he was found to have a nail in the index finger of his left hand. It was unclear if the nail had passed through the proximal phalanx. He was referred for left hand radiography.
The PA hand projection image shows the nail superimposed over the proximal phalanx of the left hand index finger.The oblique hand projection image shows the nail superimposed over the proximal phalanx of the left hand index finger. The lateral hand projection image shows the nail superimposed over the proximal phalanx of the left hand index finger. To establish whether the nail had passed through the proximal phalanx, the patient was asked to position his hand in the light from the LBD such that the shadow of the nail head was perfectly centred on the long axis of the nail (shadow arrowed). The resultant image is shown below. The axial nail image demonstrates that the nail has passed along the volar aspect of the finger missing the bone.





Discussion
- Nail gun injuries should be approached by the radiographer with specific objectives in mind. These objectives are to localise where the nail is and what damage it did getting there. It is basically a foreign body localisation procedure.
- If the nail has completely penetrated the skin, an entry site marker should be used.
- Centring the X-ray beam to the nail will eliminate parallax error.
- In the first case, the nail tip was within the cortex of the femur. The radiographer's aim in this case was to try and project the tip of the nail clear of the femur (to prove otherwise). The tangential view suggested that the nail was within the cortex.
- In the second case, the nail was demonstrated to be within the patient's soft tissues without performing any special dedicated views. Further imaging should only be undertaken to assess associated pathology.
- Good quality images will be required to demonstrate a subtle cortical "breakout" injury.
- There are some nail orientations that will benefit greatly from imaging with an image intensifier.
... back to the Applied Radiography home page
... back to the Wikiradiography home page