Right Upper Lobe Collapse
The Right Upper Lobe AnatomyThe plain film appearance of collapse of the upper lobes varies considerably between the right and left sides. The right side is the relatively easy diagnosis, being particularly characteristic in its appearance on the AP/PA projection image.
adapted from <a class="external" href="http://books.google.com.au/books?id=Bif0zpmEWtAC" rel="nofollow" target="_blank">By Fred W. Wright Radiology of the Chest and Related Conditions: Together with an Extensive Illustrative Collection of Radiographs CRC Press, 2002</a>
The RUL is comprised of three segments: apical, posterior, and anterior
Further information on lung anatomy here
adapted from <a class="external" href="http://books.google.com.au/books?id=Bif0zpmEWtAC" rel="nofollow" target="_blank">By Fred W. Wright Radiology of the Chest and Related Conditions: Together with an Extensive Illustrative Collection of Radiographs CRC Press, 2002</a>


Important Characteristics of all Lobar Collapse
1. Collapse and consolation can occur independently or together2. Collapse can be partial or complete3. It is often not clear to what extent the appearance is due to collapse or consolidation or both. The degrees of each are often unclear.4. If a lobe is only partially collapsed and there is no accompanying consolidation, there may be no increase in opacity5. In cases of pure collapse, only when the collapse is virtually complete will there be a significant increase in density of the affected lung
Radiographic Technique
It is sometimes useful to perform an apical lordotic view to help demonstrate equivocal pathological appearances in the upper lobes. It is also advantageous to direct patients to cross their arms across their heads for the lateral view (as opposed to hands on head and elbows forward). The upper lobes are frequently partially obscured by upper arm soft tissues on the lateral view when the hands on head, elbows forward technique is used.
Plain Film Appearance
The Right Upper Lobe (RUL) collapses in a manner that is similar to closing a fan.
- The horizontal fissure is attached near the hilum. As the RUL collapses it tends to close like a fan attached at the hilum.
- The horizontal fissure often is bowed.
- In cases of extreme collapse, the lobe may be indistinguishable from the upper mediastinum
A similar pattern is seen on the lateral chest image. The hilum is now in the centre of the image and the hilum collapses from both an anterior and posterior direction. The sperior half of the oblique fissure is displaced anteriorly.


As the RUL collapses a "V" shaped opacity is seen in the right apical region. The RUL collapse results in a movement of the horizontal fissure that has been likened to closing a fan.


Notes
<a class="external" href="http://www.ajronline.org/cgi/reprint/177/4/869.pdf" rel="nofollow" target="_blank">Eli Konen et al, Prevalence of the Juxtaphrenic Peak After Upper Lobectomy,
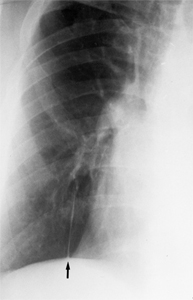
AJR:177, October 2001</a>A peak-like shadow along the medial aspect of the right hemidiaphragm is evident in some cases and is referred to as a "juxta-phrenic peak." This finding is more common in left upper lobe collapse, however. The formation of the peak is thought to be related to traction on the basal pleura by the inferior pulmonary ligament. It has also been ascribed to upward retraction of the inferior accessory fissure or an intrapulmonary septum associated with the pulmonary ligament [9]. In severe cases the RUL becomes pancaked against the lung apex or upper mediastinum and can be mistaken for apical pleural thickening. <a class="external" href="http://www.auntminnie.com/index.asp?sec=ser&sub=def&pag=dis&ItemID=53572" rel="nofollow" target="_blank">Scott Williams, Aunt Minnie, April 3, 2002</a> S Sign of Golden - This sign refers to a reverse "S" shape that the minor fissure takes on in cases of RUL collapse resulting from a central obstructing mass. The superior portion of the "S" is from the displaced minor fissure, while the inferior portion results from the mass itself. The sign is commonly seen, but it is neither sensitive nor specific for lung cancer. <a class="external" href="http://www.radiologynotebook.com/atelectasis.html" rel="nofollow" target="_blank">http://www.radiologynotebook.com/at</a><a class="external" href="http://www.radiologynotebook.com/atelectasis.html" rel="nofollow" target="_blank"> </a><a class="external" href="http://www.radiologynotebook.com/atelectasis.html" rel="nofollow" target="_blank">electasis.html</a>




<a class="external" href="http://www.ajronline.org/cgi/reprint/177/4/869.pdf" rel="nofollow" target="_blank">
</a>With marked collapse of the RUL, the density of the lobe may blend with that of the right superior mediastinum
Felson, Benjamin (Chest Roentgenology, W.B. Saunders, 1973, p38)
for a more extreme example -
<a class="external" href="http://bjr.birjournals.org/content/vol74/issue877/images/large/BI72386.8.1.jpeg" rel="nofollow" target="_blank">http://bjr.birjournals.org/content/vol74/issue877/images/large/BI72386.8.1.jpeg</a>
<a class="external" href="http://www.auntminnie.com/index.asp?sec=ser&sub=def&pag=dis&ItemID=53572" rel="nofollow" target="_blank"> </a>

... back to the Applied Radiography home page