Pneumothoraces
Causes of PneumothoraxPneumothorax is a commonly encountered chest pathology in most Emergency Departments. This page considers the pathological appearances of pneumothorax and the radiographic techniques employed to demonstrate them..
- spontaneous
- trauma
- iatrogenic
- Asthma
- Catamenial
- Alpha 1 antitrypsin deficiency
Inspiration and Expiration Views
A commonly employed radiographic protocol for pneumothorax detection is to perform inspiration and expiration PA/AP erect chest radiography. It is noteworthy that the expiration image can be useful for detection because the pneumothorax is likely to increase in size. The inspiration image is required for measurement of the pneumothorax i.e. sizing. Compare the size of the penumothorax (arrowed) on this expiration radiograph compared with the inspiration radiograph above.


Erect vs Supine Pneumothorax
Supine PneumothoraxWhy should the plain film appearances of pneumothorax be different for erect and supine images? The answer has everything to do with gravity. The lung affected by the pneumothorax is partially free to move under the effects of gravity because it is not limited by the normal constraints of the uncompromised pleural space. A lung which has been compromised by pneumothorax will tend to fall into the most dependent position in the thoracic cavity.
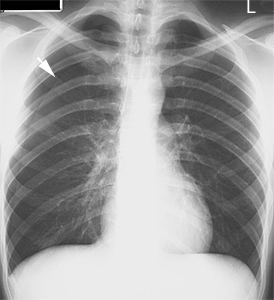
Erect Position
In the erect position the lung will tend to fall towards the diaphragm. This is why the pneumothorax is often most evident at the lung apex (arrow). Note that the lung is attached at the hilum and will therefore tend to collapse inferiorly and medially in the erect position.
In the supine position the lung will tend to fall to the posterior chest wall. The pneumothorax will usually be evident near the diaphragm first.




What to Look for
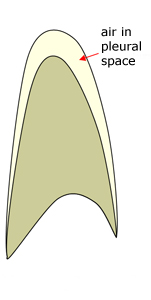
As the diagram above suggests, in the supine position, air in the pleural space will tend to collect anteriorly and inferiorly. Tocino (<a class="external" href="http://radiographics.rsnajnls.org/cgi/content/abstract/5/4/557" rel="nofollow" target="_blank">http://radiographics.rsnajnls.org/cgi/content/abstract/5/4/557 </a>)describes the situation as follows
"In the supine position, the anteromedial space becomes the least dependent
pleural recess. Air in this space may reveal the earliest and, often,
most subtle radiographic signs of pneumothorax. As the volume of air in-
increases, signs of pneumothorax will extend into the subpulmonic space and
then into the apicolateral space.
The anteromedial space is divided by the hilar structures into superior
and inferior compartments. Initially, air will accumulate preferentially in one
of these compartments. Air in the superior anteromedial space accounts for
the sharp delineation of mediastinal contours ...... . In fact, air interposed
between abnormal lung parenchyma and the mediastinal structures
(absence of the silhouette sign) should raise suspicion of pneumomediastinum
or pneumothorax."
Signs of Supine Pneumothorax
Sign Description 1 Etched Diaphragm Diaphragm contrasted with air in pleural space 2 Etched Mediastinum Mediastinum (heart border) outlined with air in the pleural space 3 Deep Sulcus Sign Abnormally prominent/deep costophrenic angle 4. Visible Visceral Pleura Most often seen as a doublediaphragm-like appearance 5. Mediastinal shift As in the erect position, mediastinal shift may indicate the presence of a pneumothorax under tension 6. Uneven Lung Density Affected lung may appear abnormally translucent. Abnormal lung may also appear abnormally opaque in hydropneumothorax from veiling density 7. Absent Lung Markings This will usually occur in the presence of other signs 8. Subcutaneous Emphysema Associated with rib fracture
Radiographic Technique
The supine pneumothorax is best demonstrated on full expiration. A caudally angled image centred on the diaphragm may be of some assistance in the presence of a subpulmonic pneumothorax. A supine cross-table lateral chest may provide further evidence of pneumothorax by displaying air accumulated anteriorly in the pleural space. An apical lordotic view may also help to demonstrate a pneumothorax but is more likely to be of assistance with the patient in the erect position.
If the patient is able to be imaged in the erect position this will clearly be advantageous.
Spontaneous Pneumothorax
This 20 year old male presented to the Emergency Department with chest pain. He was examined and referred for chest radiography.
There is a left sided pneumothorax visible at the lung apex.The pneumothorax is arrowed
azygos lobe notedA magnified image demonstrates the visceral pleura to have an irregular margin. This irregular margin is likely to represent underlying apical subpleural blebs. Apical Subpleural Bleb
<a class="external" href="http://www.rtso.ca/themes/acquia_marina/student/pneumo.htm" rel="nofollow" target="_blank">
http://www.rtso.ca/themes/acquia_marina/student/pneumo.htm</a> (1/2/2011)The stereotypical Spontaneous pneumothorax patient is a young, tall, thin male with no history of medical problems. The predominance of SP in men is overwhelming; SP affects 5-10 times as many males as females. The peak age group is 20-29 years of age, and many studies indicate much higher susceptibility among smokers, though some studies dispute this claim. The harmful ingredients in tobacco smoke may irritate the pleura and therefore increase the likelihood of a rupture or tear in the pleural membrane. The reason for the high incidence of spontaneous pneumothorax among tall males is not completely understood. However, many feel that the morphology and physiology of tall men is such that they have an inherent defect in their structure which is manifested by a lengthened chest cavity and lung. This structure makes the lung apex more vulnerable to gravitational and other stresses which may cause bleb formation and a subsequent spontaneous collapse of the lung. In addition to body structure, other risk factors for the development of SP are pre-existing lung disease, the presence of sub pleural blebs, and forceful coughing. When evaluating patients reporting chest pain, one must always consider SP if the patients are tall, thin, young men with a positive smoking history.
<a class="external" href="http://www.pilotfriend.com/aeromed/medical/pneumothorax.htm" rel="nofollow" target="_blank">http://www.pilotfriend.com/aeromed/medical/pneumothorax.htm 1/2/2011</a>Bleb or Bulla? Spontaneous pneumothorax occurs when air enters the pleural space in the absence of a traumatic or iatrogenic cause. The most common source of air is the lung parenchyma with the most common cause being pulmonary blebs or bullae. Pulmonary blebs are accumulations of air within the layers of the visceral pleura that form when air escapes from within the lung parenchyma and travels to the lung surface, most commonly the lung apices. In contrast, pulmonary bullae are air-filled spaces within the lung parenchyma that result from the destruction, dilatation, and confluence of adjacent alveoli.
<a class="external" href="http://cat.inist.fr/?aModele=afficheN&cpsidt=15142295" rel="nofollow" target="_blank">quoted from http://cat.inist.fr/?aModele=afficheN&cpsidt=15142295</a> 1/2/2011






The Importance of Subcutaneous Air
Case 1
This 40 year old male presented to the Emergency Department after falling off a ladder. He was examined in the ED and referred for chest and thoracic spine radiography.
There is evidence of subcutaneous emphysema adjacent to the right hemidiaphragm. It is important to ask where this air might have come from. There are two sources of air in close proximity- one is the ambient air (outside the skinline) and the other is in the lung. If there is no skin laceration, you can usually eliminate the ambient air as a source. This leaves the lung as the source of the subcutaneous air. For the lung to be a source of this subcutaneous air, the pariental and visceral pleura would need to be compromised. In the presence of trauma, this is often the result of a rib fracture(s). A pneumothorax should be assumed to be present until proven otherwise. It would be prudent to keep this patient in ED or admit the patient to monitor this injury. The danger in discharging this patient from ED is that they will re-present with a large pneumothorax (usual haemopneumothorax).
Further plainfilm imaging or ultrasound fastscan may assist in assessing the presence/size of the pneumothorax.The radiographer proceeded to perform rib views to establish whether there was a rib fracture associated with the subcutaneous emphysema. At least one rib fracture was identified (arrowed) A magnified image demonstrates a pneumothorax. There is also likely to be a second rib fracture below the arrowed fracture.
(Incidental note- There is a suggestion of demonstration of regularly spaced interlobular septae of the secondary pulmonary lobules!)



Case 2
This 28 year old male presented by ambulance to the Emergency Department following a motor vehicle accident.
He was referred for a radiographic trauma survey.
The radiographer noted a lucent appearance adjacent to the right hemidiaphragm. This was not associated with a skin laceration. The radiographer was suspicious that this might represent subcutaneous emphysema and proceeded to perform additional imaging of the right hemithorax to include more of the axillary/chest wall soft tissuesThe lucency was again demonstrated. The patient could reasonably be assumed to have suffered a traumatic pneumothorax. The patient was discharged and represented the next day with shortness of breath. The patient was referred for chest radiography revealing a large hydropneumothorax.



Post Intercostal Drain Pneumothorax Radiography
The ideal position for an intercostal drain will depend on the position that the patient will be nursed in and the intended use of the drain. If the drain is intended to drain pleural fluid, the drain holes should be positioned posteriorly within the pleural space. If the intercostal drain is inserted to re-expand a lung in a patient with pneumothorax, the drain holes should be anterior. If the patient is being nursed in the erect position, the drain holes should also be apically positioned.
This intercostal drain is in a basal position. It is not known whether it is anterior or posterior within the pleural space.The lateral chest view image demonstrates the intercostal drain to be posterior. This is not a suitable position for lung re-expansion in a patient with a pneumothorax.
The radiographic protocol for chest radiography for new intercostal drain (or changed position) should include a lateral view where practicable.


Flail Chest
source: unknownFlail chest refers to a condition in which there are two or more adjacent pairs of rib fractures. The adjacent pairs of rib fractures form a segment a chest wall that is able to move independently. When the patient breathes in this segment will move in a paradoxical manner. A segment of the chest wall that is flail is unable to contribute to lung expansion. These videos demonstrate the paradoxical movement of the flail segment of chest wall. Note that the flail segment of chest wall moves "in" on inspiration and "out" on expiration. This appearance can be clearly seen on some patients but tends to be hidden on larger patients. This 3D CT reconstruction demonstrates multiple pairs of ribs fractures on the left producing a flail segment of chest wall.


Loculated pneumothorax
A loculated pneumothorax is a pocket of pleural air trapped in a localised area. The plain film appearances may be subtle. This patient underwent CT guided biopsy of a right lung lesion. The black arrow identifies a loculated pneumothorax. The expiration erect PA post-biopsy chest image above demonstrates the loculated pneumothorax as a subtle vertical line (arrowed)
Note that the CT scan was performed with the patient in a PA position- this is the right lung.


False Pneumothorax from Skin Folds.
This is a radiograph rather than a digital image.
The arrowed structure could easily be mistaken for a pneumothorax. It is actually a skin fold on the patient's back. Skin folds such as this are a result of the contact between the patient's skin and the IR (in this case a cassette). The chance of producing a skin fold such as this is increased when the patient has loose skin (typically elderly patients and/or patients who have lost weight) and when the cassette is repositioned with the patient skin in contact with the cassette.
Radiographers should be aware of the appearance of skin folds simulating pneumothorax and the cause of the appearance. Where a skinfold is suspected, close examination of the image will usually reveal lung markings 'beyond' the skinfold.This is a radiograph rather than a digital image.
The arrowed structure could be mistaken for a pneumothorax but is actually a skinfold.There is a pneumothorax (top arrrow), axillary skin fold (middle arrow), and breast shadow (bottom arrow).



Pneumothorax or Bulla(e) or Both?
This patient has overexpanded lung associated with emphysema. The white arrowed structure is a bulla. This is an abnormal airsac within the lung. The patient also has a pneumothorax (black and white arrows). The distinction between an bulla and a pneumothorax is important- you don't want to insert an intercostal drain into a bulla mistaken for a pneumothorax. Where the distinction is not clear, supplementary views (expiration , decubitus) may be helpful.

This patient was referred for chest radiography following a right subclavian line insertion. The radiography was performed supine in ICU with a CR cassette inserted underneath the patient. The arrowed structure appears at a cursory glance to be a pneumothorax. On closer inspection, the line neither continues to extend superiorly nor inferiorly. There is also evidence of lung markings beyond the apparent pneumothorax (beyond the apparent lung border). A skin fold can often be identified by the presence of lung markings extending across the linear opacity that would otherwise represent the edge of the lung in a patient who had a true pneumothorax. The distinction between a pneumothorax and skinfold can be subtle. It is not until you place the two appearances next to each other that the distinction becomes a little clearer. What you are looking at with pneumothorax could be thought of as reverse silhouette sign. The lung edge/visceral pleura has a sharply marginated etched appearance due to the contrast with the air in the pleural space. By contrast, a skin fold is an artifact superimposed on lung parenchyma and does not demonstrate that sharp clearly marginated appearance of a true pneumothorax.
Other considerations are that a false pneumothorax line will tend to fade out at both ends. Also, related to the discussion above, lung markings will generally not cross the apparent lung edge in cases of true pneumothorax (exceptions may occur depending on the collapsed shape of the lung).
It should also be remembered that pneumothorax is not just a radiographic diagnosis (some would argue that it is primarily a clinical diagnosis) - evidence of pneumothorax by auscultation (stethoscope sounds) and other clinical evidence should be taken into consideration. Medical imaging is often thought of as providing a positive or negative answer to the clinical question- this is a fundamental misunderstanding of the nature of medical imaging.



Iatrogenic Pneumothorax
The term iatrogenic refers to any pathology induced inadvertently by a physician or surgeon or by medical treatment or diagnostic procedures. Etymologically, the term means "brought forth by a healer" (iatros means healer in Greek); as such, in its earlier forms, it could refer to good or bad effects. <a class="external" href="http://en.wikipedia.org/wiki/Iatrogenesis" rel="nofollow" target="_blank">(http://en.wikipedia.org/wiki/Iatrogenesis)</a>
Apical Lordotic ViewAssociated with NGT Insertion
This NGT has taken a path down the right main bronchus then made its own path through lung parenchyma into the pleural space.
This NGT was removed from the pleural space and replaced with an underwater sealed drain (UWSD) which was inserted percutaneously.
The pneumothorax is not demonstrated but is known to exist given the course of the NGT

This patient was involved in a MVA and received trauma to the right chest. There was some question as to the presence of a right pneumothorax and a suggestion that the right lung was slightly more hyperlucent than the left. This is the erect PA chest image. The radiographer performed an erect apical lordotic view to show the patients lung apices without the superimposed clavicle. No pneumothorax was demonstrated.


False Pneumothorax from Breast/Axillary Soft Tissue Lines
There are several soft tissue lines demonstrated. Do they represent pneumothoraces? These lines are axillary/breast soft tissues (arrowed)


... back to the wikiradiography home page
... back to the Applied Radiography home page